PAC-MAN
Pulmonary Artery Catheters in patient Management
PAC-MAN study group, Lancet 2005;366;472-477
Clinical Question
- In critically ill patients, does the use of a pulmonary artery catheter (PAC) reduce mortality?
Design
- Randomised controlled trial
- Non-blinded
- Stratified by age and presumptive clinical syndrome
- Intention to treat analysis
- Power calculation: 1281 patients would allow detection of a 10% change in absolute hospital mortality, with a 5% false positive rate and a 10% false negative rate
Setting
- 65 ICUs in the UK
- 13 university, 8 university affiliated, and 44 non-university hospitals
- October 2001 – March 2014
Population
- Inclusion: adult patients admitted to the ICU who the treating clinician felt should be managed with a PAC
- 66% medical, 6% elective surgery, 27% emergency surgery
- 13% acute respiratory failure, 66% multiorgan dysfunction, 11% decompensated heart failure
- 1st 24hr APACHE II total score 22.4 (mean)
- Exclusion: elective admission for preoperative optimisation, presence of a PAC on admission to the ICU, haemodynamic optimisation before organ donation
- 1041 patients randomised
Intervention
- Use of a PAC
- Median time from randomisation to PAC insertion was 1.7hrs, total number of days that PAC was indewlling was 3 (2-4) days
- In patients treated with a PAC, 80% had 1+ changes in clinical management within 2hr of insertion as direct result of PAC-derived data
- fluid bolus >200ml (42%)
- change in dose of vasoactive drug >25% (43%)
- introduction of vasoactive drug (32%)
- 34/519 (7%) were not managed with a PAC due to unsuccessful insertion, change in clinical condition or coagulopathy
Control
- PAC not used
- units decided prior to study commencing to have no option of alternative cardiac output monitoring device (21%) or to retain the option of using another cardiac output monitoring device (79%)
- 24/522 (5%) of patients were managed with a PAC due to loss of equipose
Outcome
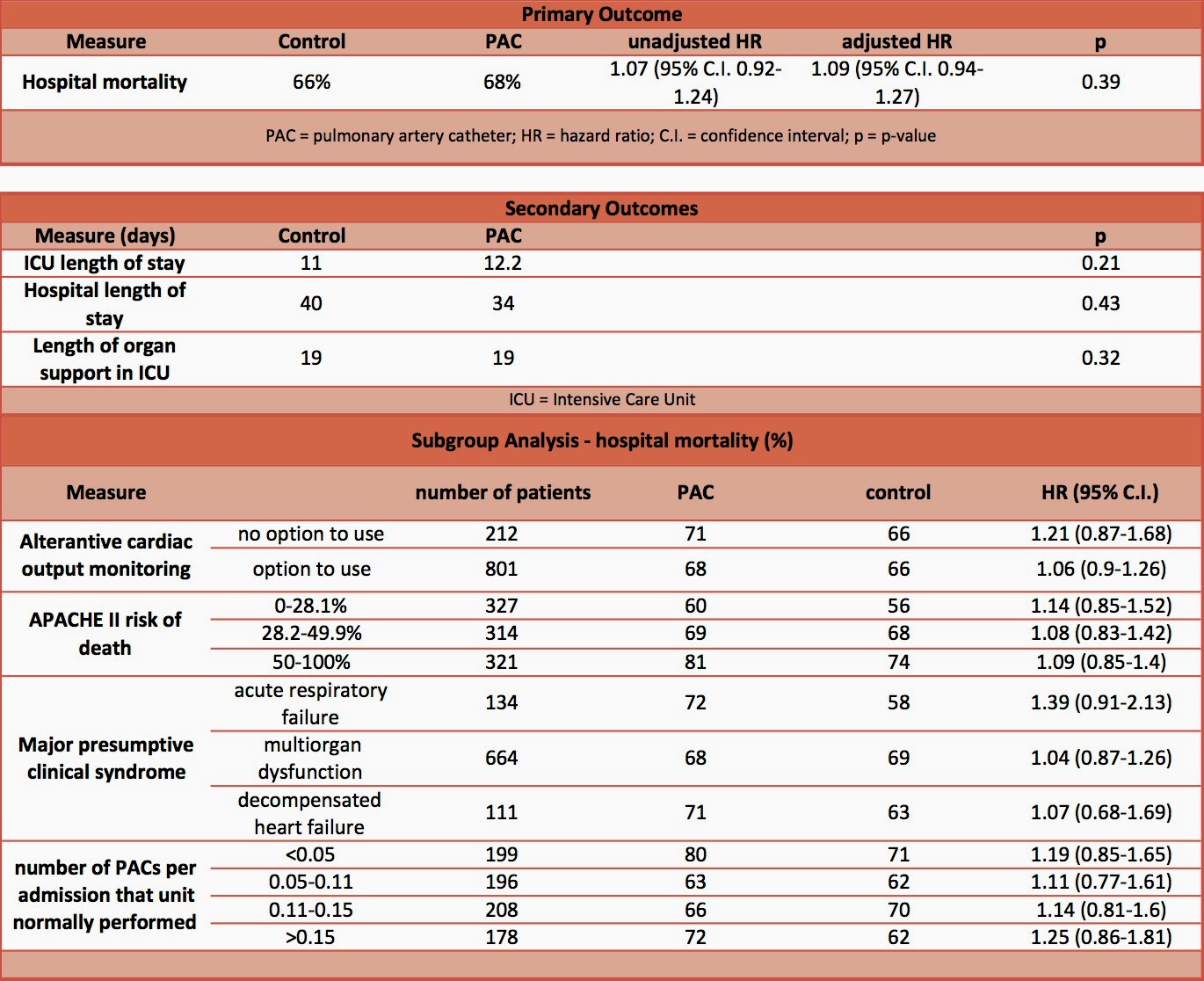
- Primary outcome: hospital mortality – no significant difference
- 66% in control vs. 68% in PAC, p=0.39
- Secondary outcome
- No significant difference in:
- ICU length of stay
- Hospital length of stay
- Number of days of organ days in ICU
- No significant difference in:
- direct complication reported in 46 (10%) patients in whom PAC insertion attempted
- haematoma at insertion site, n=17 (4%)
- arterial puncture, n=16 (3%)
- arrhythmias needing treatment within 1hr of insertion, n=16 (3%), one of which was a cardiac arrest
- pneumothoraces, n=2
- haemothorax, n=1
- retrieval of lost insertion guidewire, n=2
- Sub-group analysis
- no significant difference based upon APACHE II score, major presumptive clinical syndrome, or whether units had no option of alternative cardiac output monitoring or retained option of cardiac output monitoring, or whether unit had historical high (>15%) or low (<5%) rate of PACS/admission
Authors’ Conclusions
- No clear benefit or harm from the use of PAC in critically ill patients
Strengths
- Randomised
- Multi-centre
- Intention to treat analysis
- Pragmatic study, with wide inclusion criteria, investigating if there is a benefit from how a PAC was used in everyday practice. The downside to this is that there was no set protocol and therefore the patients included in the trial could have been managed with a number of different strategies, some of which may have been beneficial while others harmful.
Weaknesses
- Did not assess quality of use of PAC. The authors highlight the high degree of ignorance amongst ICU staff when it come to interpreting data from a PAC
- Did not assess for late-onset complications e.g. infection
- Use of ultrasound not reported. This is likely because it was not used. If it had been used then the number of complications may have been reduced
- Not powered for subgroup analyses. I am most interested in whether or not PACs are useful for decompensated right heart failure or pulmonary hypertension. Other less invasive cardiac output monitoring devices will provide sufficient haemodynamic indices in non cardiogenic shock
The Bottom Line
- In units that practice PACs on a regular basis for critically ill patients, there was no benefit found from the use of a PAC. Complications occurred in 10%, although some of these may have been avoided with the use of ultrasound. Subgroup analysis showed no benefit in any ‘major presumptive clinical syndrome,’ however like with all studies, subgroup analyses were not sufficiently powered to give us the definite answer.
- Historically, the majority of ICUs that took part in the study used PACs frequently. Current practice means that a number of units use PACs very infrequently, much less than 5% which was the cut-off in the study for ‘low use of PAC’. With unfamiliarity the benefits from the use of a PAC may be less and the complications may be greater.
External Links
- [article abstract] Assessment of the clinical effectiveness of pulmonary artery catheters in management of patients in intensive care (PAC-Man): a randomised controlled trial
- [article abstract] Post-hoc analysis
- [Podcast] Charming the yellow snake, Ray Rapper, ICN & SMACC
- [Commentary] Obituary: pulmonary artery catheter 1970 to 2013, Marik
Metadata
Summary author: @davidslessor
Summary date: 10.08.2014.
Peer-review editor: @DuncanChambler