TARGET
Energy-Dense versus Routine Enteral Nutrition in the Critically Ill
Chapman M, Peake S: NEJM 2018 379;19 2018:1823-1834. doi:10.1056/NEJMoa1811687
Clinical Question
- In mechanically ventilated, critically ill patients receiving enteral nutrition does energy-dense feed (1.5kCal/ ml) compared with routine feed (1kCal/ml) impact on 90 day all cause mortality?
Background
- Nutrition for critically ill patients is vital. The optimal route of delivery and optimal caloric targets has been a controversial subject over many decades
- We know:
- Enteral nutrition is preferable to parenteral nutrition (reduced chance of gastric erosion, bacterial translocation and infectious complications)
- Early establishment of feeds is desirable but not always possible
- It is difficult to achieve caloric goal targets, due to the complex nature of the intensive care patient with interruptions in feeds for procedures, high gastric aspirates, vomiting etc
- The research to date has not answered what we should aim for in regards to caloric targets.
- Some trials have examined early trophic feeding (~400kcal/day): EDEN RCT, some have examined standard calories (~1300kcal/day) and some have studied energy-dense nutrition (~1900kcal/day) ACCEPT trial. There have been little or no differences in mortality and other outcomes between control and intervention groups in these trials
- Guidelines (Canadian CC, ESPEN and ASPEN) have offered advice regarding caloric goals and have erred on the side of higher energy targets. (25-30kcal/kg/day ~1900-2200cal/day)
Design
- TARGET: The Augmented versus Routine approach to Giving Energy Trial
- Multicentre, double-blind, RCT
- 1:1 assignment to groups using permuted block randomisation, variable block size, site stratification
- Allocation concealment achieved by web-based randomisation
- Blinding achieved by indistinguishable packaging between the energy-dense and routine feeds
- A sample size of 3774 provided 80% power to detect a difference of 3.8-4.3 percentage points in 90-day mortality assuming a baseline mortality of 20-30%. Sample size was increased to 4000 to allow for loss of follow-up
- Analyses was by modified intention to treat
Setting
- 46 ICUs in Australia and New Zealand
- June 2016 to November 2017 (with 90 day follow-up)
- 4000 were randomised
- 26 in high energy group and 17 in routine group were excluded from the modified ITT evaluation due to withdrawal of consent, not meeting all inclusion/exclusion
- 23 in high energy group and 20 in routine group were excluded due to later withdrawal of consent or loss to follow-up
- 3914 patients were available for analysis of the primary outcome
Population
- Inclusion: All ICU patients, 18 years and older, invasively ventilated and expected to be requiring enteral nutrition until at least the day after randomisation
- Exclusion: patient had already received EN or PN >12 hours in this ICU admission, treating team felt 1ml/kg contraindicated, death deemed imminent, burns >15%
- Patients well matched at baseline, particularly with similar APACHE II scores and requirements for organ support
Intervention
- Energy dense feed
- Target rate of 1ml/kg of 1.5kcal/ml of enteral feed based on ideal body weight (~1900kcal/day)
Control
- Standard feed
- Target rate of 1ml/kg of 1kcal/ml of enteral feed based on ideal body weight (~1300kcal/day)
Management common to both groups
- The feeds differed in caloric content achieved by higher fat and carbohydrate in the energy dense feed but there was similar protein content in the 2 feeds
- Other management was at the discretion of the treating teams
Outcome
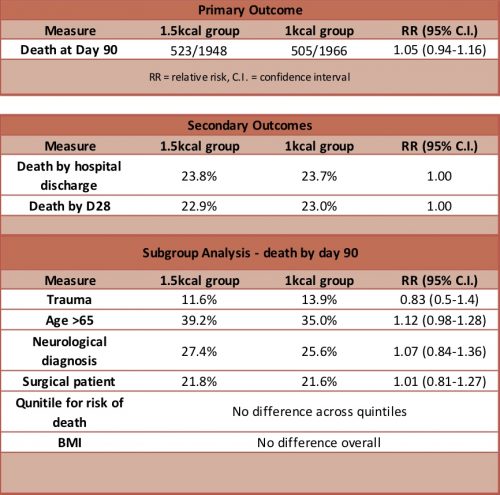
- Primary outcome: All cause 90-day mortality: 1.5kcal/ml vs 1kcal/ml; no difference
- 523/1948 (26.8%) vs 505/1966 (25.7%) [RR 1.05; 95% CI, 0.94-1.16, p=0.41]
- Secondary outcome: no difference in any secondary outcome
- Survival time
- 90-day cause specific mortality
- ICU-free and hospital-free days (until D28)
- Days free of organ support (until D28)
- % ventilated, vasopressors or new RRT (D28)
- % with Positive blood cultures
- Antimicrobials received between randomisation & D28
- Seven pre-specified subgroups:
- Age >65
- Trauma
- Sepsis
- Neurological
- Medical vs Surgical patients
- Quintiles for absolute risk of death
- BMI
- GI tolerance and metabolic effects
- Gastric residual volumes were significantly higher in the high energy group (250ml vs 180ml)
- Regurgitation and vomiting were more prevalent in the high energy group (19 vs. 16%)
- The use of insulin was more prevalent in the high energy group (56 vs 49%)
- Prokinetic drug use was more prevalent in the high energy group (47 vs 40%)
Authors’ Conclusions
- Energy dense enteral nutrition did not improve 90-day survival amongst ventilated ICU patients
Strengths
- Multicentred, double-blinded, allocation concealment, good follow-up, intention-to-treat- analysis
- Clinically meaningful outcomes
- Prespecified subgroups
- Addresses a clinically important question and is the largest critical care nutrition trial ever undertaken
Weaknesses
- Only 2% of patients were malnourished as assessed by BMI. The generalisability of this study to this patient group is difficult to make
- The trial was conducted only in Australia and NZ making the extrapolation to ICUs in other settings, eg developing countries, challenging
- Protein intake was the same between groups. There is no assessment of the value of hyperproteinemic feeds
- Clinically important subgroups were predefined but a heterogenous ICU population does not exclude a benefit of different caloric targets in certain groups that was not detected in this study (either because no difference exists or the study was not powered to detect the difference in these subgroups)
- The caloric targets were calculated using ideal body weight. The evidence is scant, but some would advocate that calorimetry assessing energy expenditure should be the gold standard in these patients
The Bottom Line
- This trial provides reassurance to me that my usual practice of providing 1ml/kg (actual weight) of standard feed (1kcal/ml) is safe for my mechanically ventilated ICU patients
- My patient may also receive some calories from propofol, citrate dialysis and dextrose infusions but this is unlikely to alter outcomes greatly
- I look forward with interest to the results of the 6-month quality of life follow-up for these patients which is yet to be published
External Links
- [article] Energy-Dense versus Routine Enteral Nutrition in the Critically Ill
- [further reading] What should we target after TARGET? Paul Young et al
- [further reading] Interview with authors at ESICM Paris
- [podcast] Top 5 nutrition studies – Emma Ridley presentation at ICS State of the Art Meeting, Dec 2018
Metadata
Summary author: Celia Bradford
Summary date: January 10th 2019
Peer-review editor: David Slessor


