MACMAN
Video Laryngoscopy vs Direct Laryngoscopy on Successful First-Pass Orotracheal Intubation Among ICU patients
Lascarrou, JB et al. JAMA 2017; 317(5): 483-403. don: 10.1001/jama.2016.20603
Clinical Question
- In intensive care patients requiring orotracheal intubation, does video laryngoscopy (VL) compared to the Macintosh direct laryngoscope (DL) increase the frequency of first pass intubation?
Design
- Non-blinded, multicentre, open-label, 2 parallel group RCT
- Randomisation in blocks of 4, balanced and stratified by centre and experience of intubators (“experts” vs “non-experts”)
- “Experts” – 5 years of ICU experience OR 1 year of ICU and 2 years of anaesthesia experience.
- “Non-expert” – All others
- Randomisation sequence generated by blinded statistician
- Computerised allocation provided full concealment
- Both intention to treat and per protocol analyses performed
- Missing data was considered a failed first pass intubation
- 370 participants planned, assuming first pass success rate of 65% with DL, increased to 80% with VL, type I error of 5%, and type II error of 10%
Setting
- 7 ICUs in France
- May – December 2015
Population
- Inclusion:
- ICU admission and need for orotracheal intubation to facilitate mechanical ventilation
- Exclusion:
- Contraindications to oral intubation, e.g. unstable C-spine
- Insufficient time to include and randomise, e.g. cardiac arrest
- Age <18
- Pregnant or breastfeeding
- Correctional facility inmate
- Under guardianship
- Without health insurance
- Refusal by patient or next of kin
- Previous enrolment in an RCT with intubation as the primary end point
- 489 patients screened, 371 randomised
- 186 randomised to VL, 185 randomised to DL (ITT analysis)
- 183 received VL as intended, 182 received DL as intended (per protocol analysis)
- Baseline statistics similar between groups
Intervention
- McGrath MAC Videolaryngoscope (without stylet)
Control
- Macintosh direct laryngoscope with either a 3 or 4 blade
Standard to both groups:
- All physicians in all centres were trained in the use of all equipment on mannequins before starting the studyI All “non-experts” were supervised by an “expert” during the study
- Preoxygenation with device of the intensivist’s choosing
- Non-rebreathe mask of at least 15L/min for >3 mins
- NIV with 100% oxygen for at least 3 mins
- High flow nasal cannula oxygen at 60L/min with 100% oxygen for at least 3 mins
- IV induction with EITHER etomidate 0.2/0.3mg/kg OR ketamine 1-2mg/kg
- Muscle relaxation with suxamethonium 1mg/kg OR rocuronium 1mg/kg (if sugammadex immediately available)
- Cricoid pressure was at user’s discretion
- If first pass failed, individual was allowed to choose between repeat laryngoscopy or alternative device as per French difficult airway guidelines
Outcome
- Primary outcome: Successful first pass intubation, as defined by capnography over 4 breaths or more – no significant difference
- VL 67.7% vs DL 70.3%, absolute difference -2.5%, P= 0.60
- Predefined Secondary outcomes:
- Proportion of patients with successful intubation at any attempt – no significant difference
- Total time to successful intubation – no significant difference
- Proportion of patients with difficult intubation – no significant difference
- Proportion of patients intubated with alternative techniques – no significant difference
- Duration of mandatory ventilation – no significant difference
- ICU length of stay – no significant difference
- Hospital length of stay – no significant difference
- ICU mortality – no significant difference
- 28 day mortality – no significant difference
- Cormack and Lehane grade of glottic visibility, % of glottic opening scores, reasons for intubation failure, and severe life threatening complications were significantly different between groups:
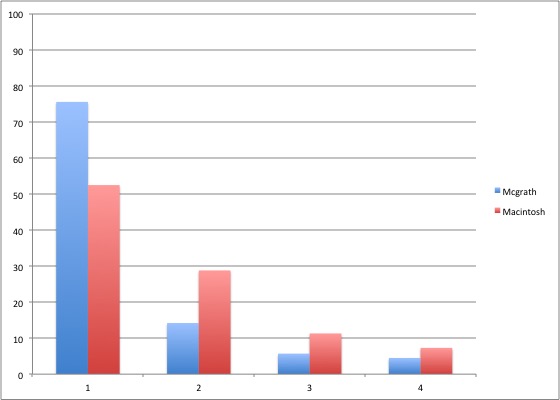
Chart of laryngoscopy view, comparing VL with DL
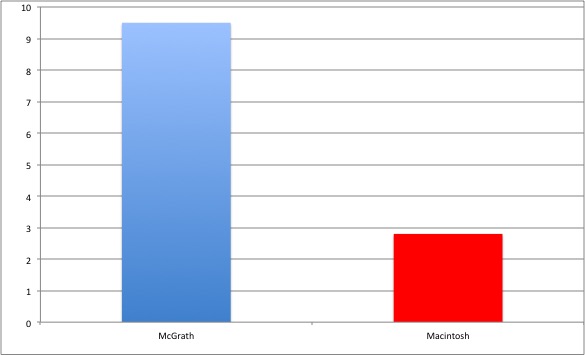
Chart of severe life threatening complications (composite of death, cardiac arrest, severe cardiovascular collapse, and severe hypoxaemia), comparing VL with DL
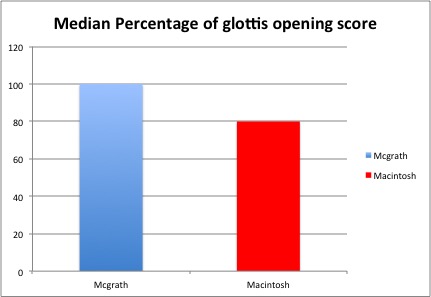
Chart of glottic opening score, comparing VL with DL
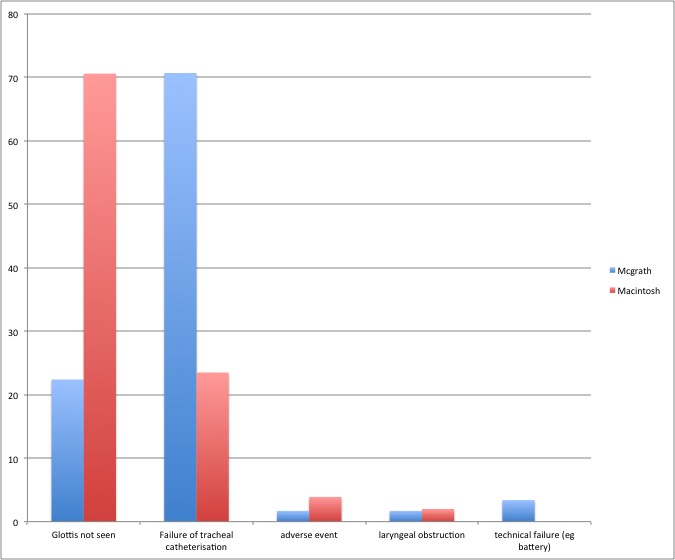
Chart of reason for intubation failure, comparing VL with DL
Authors’ Conclusions
- Amongst patients in ICU requiring intubation, video laryngoscopy compared with direct laryngoscopy did not improve first pass orotracheal intubation rates and was associated with higher rates of severe life-threatening complications
Strengths
- Important clinical question
- Accurate power calculation
- Appropriate methodology with good efforts to minimise bias, such as concealed allocation, maintenance of intended intervention and intention-to-treat analysis
- Objective, patient centred primary outcome
- Registered with clinicaltrials.gov
- All users were familiar with the devices, improving internal validity
Weaknesses
- The intubation protocol allowed for some user variability – this could affect both internal and external validity
- Suxamethonium 1mg/kg was used in the vast majority of intubations – some would debate this would not give optimal conditions for intubation (1.5mg/kg may be better (Naguib et al, 2006)
- Etomidate/sux were used in the vast majority (75-80%) of intubations – this is not common practice worldwide and reduces external validity
- The McGrath is one of many video laryngoscopes
- This trial is really a comparison of the McGrath and the Macintosh, and not a global view of VL versus DL
- In a unit where the McGrath is not the video laryngoscope of choice, I would question the applicability of these results
- The glottic view was significantly improved with the McGrath, however the intubation success was the same – there may have been an issue with technique or training
The Bottom Line
- In this trial comparing the McGrath VL and the Macintosh DL in intubating intensive care patients, there was no difference seen in the primary outcome of first pass success rate
- An association was seen with improved glottic view, and with a worsening of severe complications – however these are secondary outcomes that the study is not powered for and thus hypothesis generating only (and this is clearly stated by the authors in the paper)
- I will focus on gaining expertise with my local devices and protocols, and encouraging my team members to do the same
External Links
- [article] Lascarrou JB et al. Video Laryngoscopy vs Direct Laryngoscopy on Successful First-Pass Orotracheal Intubation among ICU patients. A Randomised clinical trial. JAMA 2017; 317 (5): 483-493 (abstract only)
- [Editorial] O’Gara B et al. Video Laryngoscopy in the Intensive Care Unit. JAMA 2017; 317(5):479-480 (abstract only)
- [Review] Lewis SR et al. Videolaryngoscopy versus direct laryngoscopy for adult patients requiring tracheal intubation. Cochrane Database of Systematic Reviews 2016, Issue 11. Art. No.: CD011136. DOI: 10.1002/14651858.CD011136.pub2. (free full text)
- [Further reading] Silverberg MJ et al. Comparison of video laryngoscopy versus direct laryngoscopy during urgent endotracheal intubation: A randomised control trial. Crit Care Med 2015; 43(3):636-641 (abstract only)
- [Further reading] ICU Revisited. Video Laryngoscopy vs Direct Laryngoscopy. Fooled eyes
Metadata
Summary author: Segun Olusanya
Summary date: 7 April 2017
Peer-review editor: Duncan Chambler



Pingback: The Bottom Line: Video Laryngoscopy vs Direct Laryngoscopy on Successful First-Pass Orotracheal Intubation Among ICU patients – Critical Care Knowledge
Full summary of the MACMAN paper over at JournalBlog.co.uk
This was a well-designed trial with strong internal validity. VL did not improve frequency of first-pass intubation although seemingly contributed to a concerning number of life-threatening complications.
The background of the doctors in the study brings into question its external validity to the UK, where a high proportion of ITU staff have greater anaesthetic experience.
Overall, the trial suggests experience trumps technique.
If my ‘go-to’ device was a videolaryngoscope, and I could always have access to it, I would still use it. If my backup device was a videolaryngoscope, I would still consider it.
Pingback: LITFL Review 277 • LITFL • Life in the Fast Lane Medical Blog
I believe the McGrath blade is a hyperangulated blade. I therefore think the outcome could be attributable to the fact that they didn’t use a stylet during the intubation attempt, which is recommended in a number of guidelines for hyperangulated blades.
This would explain why the views with the VL were superior but lower rates of being able to pass the ETT.