SAHARA – Liberal vs Restrictive Transfusion Targets in SAH

Liberal versus Restrictive Transfusion in Aneurysmal Subarachnoid Haemorrhage
English S. NEJM 2024 DOI:10.1056/NEJMoa2410962
Clinical Question
- In patients following acute aneurysmal subarachnoid haemorrhage, does a liberal strategy of blood transfusion compared with a restrictive strategy of blood transfusion reduce unfavourable neurological outcome?
- SubArachnoid Haemorrhage Red-cell transfusion And Outcome (SAHaRA)
Background
- Anaemia is common following aneurysmal subarachnoid haemorrhage with an incidence of approximately 50% during the acute admission
- The optimal target for haemoglobin concentration in this patient group is unknown
- Proposed mechanisms of benefit of transfusion include reduction in brain tissue hypoxia with the higher Hb concentration. Influences on inflammation, local oedema, vasoactive mediators and neurotransmitter production are also possible
- The TRICC trial, published in 1999, enrolled 838 critically ill patients with anaemia (Hb<9 g/dL) to a liberal strategy (transfuse if Hb< 9 g/dL) or a restrictive strategy (transfuse if Hb <7 g/dL). The in-hospital mortality rate was significantly lower in the restrictive-strategy group (22.2% vs 28.1%, p=0.05). Only 39 patients in this trial had a primary diagnosis of a ‘neurologic abnormality’ (not necessarily SAH) making the results difficult to generalise to the SAH cohort
- This study was also conducted in an era where leukodepleted blood was not used
- There have been 3 trials published more recently which favour a liberal strategy for transfusion (although the predefined criteria for statistical significance was not met). These trials have been conducted in the era of leukodepleted blood
- The TRAIN trial: patients with mixed acute neurological injury (TBI, ICH, SAH) were randomised to a liberal strategy (transfuse if Hb < 9 g/dL) or a restrictive strategy (transfuse if Hb <7 g/dL). There was a lower rate of unfavourable neurological outcome at 180 days in the patients in the liberal strategy group (62% vs 72% in all patients and 66% vs 76% in the SAH cohort)
- The HEMOTION trial: patients with TBI were randomised to a liberal strategy (transfuse if Hb < 10g/dL) or a restrictive strategy (transfuse if Hb < 7g/dL). An unfavourable outcome occurred in 249 of 364 patients (68.4%) in the liberal-strategy group and in 263 of 358 (73.5%) in the restrictive-strategy group (adjusted absolute difference, restrictive strategy vs. liberal strategy, 5.4 percentage points; 95% confidence interval, −2.9 to 13.7)
- The MINT trial: patients with Type 1 myocardial infarction. Death occurred in 9.9% of the patients with the restrictive strategy (Hb <8 g/dL) and in 8.3% of the patients with the liberal strategy (Hb<10 g/dL) (risk ratio, 1.19; 95% CI, 0.96 to 1.47); myocardial infarction occurred in 8.5% and 7.2% of the patients, respectively (risk ratio, 1.19; 95% CI, 0.94 to 1.49)
Design
- Multicentre, parallel-group, open-label, randomised clinical trial
- 1:1 ratio of a liberal vs restrictive red-cell transfusion strategy
- Computer-generated allocation concealment with permuted blocks of 4 & 6
- Stratified to centre
- Pre-specified subgroups were age > 55 years, sex, WFNS grade, radiographic grade (modified Fisher Score), method of aneurysm securement and presence of baseline DCI or radiographic vasospasm
- Blinding of outcome assessors
Setting
- 23 centres, specialising in neurocritical care, in 3 countries (Canada, Australia, USA)
- Enrolment into a pilot trial occurred from October 2015 to November 2016, with the full trial from March 2018 to July 2023
Population
- Inclusion: patients with first episode of aneurysmal SAH, ≥18years, Hb ≤ 10g/dL, within 10 days of admission
- Exclusion: non-aneurysmal SAH, active bleeding with haemodynamic instability, contraindication to transfusion.
- Sample size: 740 patients were required to demonstrate a 25% relative improvement in the primary outcome in the liberal strategy group, based on an estimated 40% event rate in the restrictive threshold arm: 80% power, with a 2-sided type 1 error rate of 5%, allowing for 3% loss to follow-up
- 742 patients randomised
- Comparing Baseline characteristics of liberal vs. restrictive group similar:
- Mean age 59.3 vs 59.5 years
- Female: 81.7 vs 81.7%
- Well matched for other comorbidities, clinical and radiographic severity
- Median WFNS grade: 3
- 87.2% of aneurysms were in the anterior circulation
- 60.5% were secured by endovascular approach
Intervention
- Liberal Group
- Transfusion was mandatory when haemoglobin <10g/dL
Control
- Restrictive Group
- Transfusion was permitted when haemoglobin <8g/dL
Management common to both groups
- Single units of leukodepleted red cells were utilised
- The allocation was applied from time of randomisation to Day 21 after admission, death or hospital discharge (whichever came first).
- Hb checks occurred daily
- The rest of the patient care was directed by bedside clinicians
Outcome
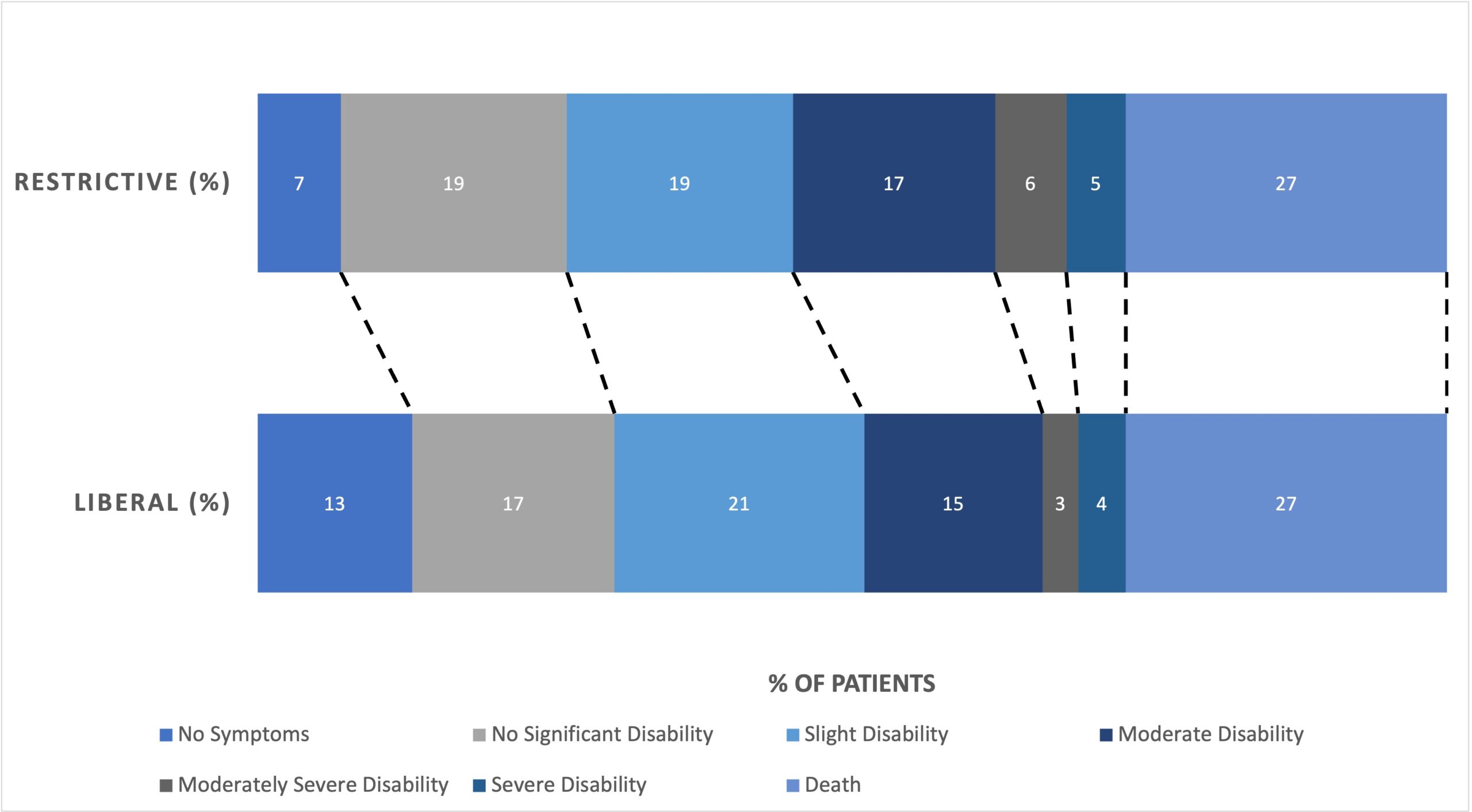
- Primary outcome: an unfavourable neurological functional outcome, defined by MRS (modified Rankin score)≥ 4 at 12 months
- MRS ≥4 at 12 months was observed in 122 of 364 patients (33.5%) in the liberal-strategy group and in 136 of 361 patients (37.7%) in the restrictive-strategy group (risk ratio, 0.88; 95% confidence interval [CI], 0.72 to 1.09; P = 0.22)
- Subgroup analysis: there were no statistically significant differences in outcomes in the predefined subgroups
- Secondary outcomes: FIM (Functional Independence Measure)
score, EuroQol-5D-5L (a quality of life score with 5 dimensions, 5 levels), VAS (Visual Analogue Score) mean score, mortality at 12 months, radiographic vasospasm, DCI, cerebral infarct - Comparing liberal vs. restrictive group
- No significant difference in
- FIM score: 82.8±54.6 vs 79.8±54.5 (mean difference, 3.01; 95% CI, −5.49 to 11.51)
- No significant difference in
- EuroQol-5D-5L: 0.5±0.4 in both groups (mean difference, 0.02; 95% CI, −0.04 to 0.09)
- No significant difference in
- VAS mean: 52.1±37.5 vs 50±37.1 (mean difference, 2.08; 95% CI, −3.76 to 7.93)
- No significant difference in
- Mortality at 12 months: 27.2% vs 27.1% (risk ratio, 0.99; 95% CI, 0.77 to 1.28)
- Lower incidence in liberal group of:
- Radiographic vasospasm: 31.5% vs 40.7% (risk ratio, 0.77; 95% CI, 0.63-0.95)
- No significant difference in
- DCI (a decrease in GCS ≥ 2 points or new focal neurological deficit ≥ 1 hour) and new infarction (on CT imaging)
- No significant difference in
- Tertiary Outcomes: comparing liberal to restrictive
- Red-cells received: median of 2 units vs 0 units
- No difference in length of ventilation, ICU LOS, hospital LOS.
- Adverse Events and Safety
- No difference between groups in transfusion reactions, thrombotic events, cardiovascular events and ARDS. No difference in infectious complications
Authors’ Conclusions
- In patients with aneurysmal subarachnoid haemorrhage and anaemia, a liberal strategy of red-cell transfusion over the first 21 days of hospitalization did not result in a lower risk of an unfavourable neurologic outcome at 12 months compared to a restrictive strategy
Strengths
- Allocation concealment, intention-to-treat analysis, near complete follow-up
- Blinding of outcome assessors
- Multicentre, multi-country improves the external validity of the results
- Balanced co-interventions
- Good adherence to protocol with low rates of protocol violations, and patients remained on the protocol for a meaningful length of time
- 17 vs 16 days
- Good separation in measured haemoglobin levels
- The authors have focused on clinically meaningful outcomes
- Further refinement of core outcome sets in people with lived experience of SAH will allow future finessing of the most important outcomes that should be measured in this patient group
Weaknesses
- The trial may well be underpowered to detect a statistically significant difference as a 25% reduction in the primary outcome is an optimistic target
- The trial used the traditional frequentist statistical technique
- A Bayesian technique may have produced a more interpretable result
- There was quite a high decline in consent
- 378 out of 1770 patients screened declined participation in the trial
- The reasons for this could be explored, but may be fear that transfusion is not safe or a distrust in medical therapies
The Bottom Line
- A liberal transfusion strategy in patients with acute aneurysmal subarachnoid haemorrhage has resulted in a signal of benefit in patient outcomes, without any evidence of harm
- The MRS at 12 months and the reduced incidence of radiological evidence of vasospasm both favour the liberal strategy
- An individual patient meta-analysis combining the results of this study and the SAH patients from the TRAIN study would add knowledge to this space
- I will aim for a haemoglobin >9g/dl in this patient group
External Links
- Liberal versus Restrictive Transfusion in Aneurysmal Subarachnoid Haemorrhage SAHaRA
- Restrictive vs Liberal Transfusion Strategy in Patients With Acute Brain Injury
TRAIN trial - A Multicenter, Randomized, Controlled Clinical Trial of Transfusion Requirements in Critical Care TRICC trial
Metadata
Summary author: Celia Bradford @celiabradford
Note a potential conflict of interest – I am a named site investigator on the paper
Summary date: December 16 2024.
Peer-review editor: George Walker
Picture by: Amine M’siouri / Pexels


