RELIEF

Restrictive versus Liberal Fluid Therapy for Major Abdominal Surgery
Myles.NEJM 2018. Published on line first on May 10, 2018 DOI: 10.1056/NEJMoa1801601
Clinical Question
- In adult patients undergoing major elective abdominal surgery, does a restrictive fluid regimen compared with a liberal fluid regimen reduce complications and improved disability-free survival?
Background
- Around 310 million patients worldwide undergo major surgery each year
- The most effective fluid regimen during surgery remains unclear but more recent studies and guidance emphasising the importance of avoiding excessive fluids
- Fluid restriction could increase the risk of hypotension and decrease perfusion to the kidneys and other vital organs leading to organ dysfunction
- Excessive intravenous fluids may increase the pulmonary complications, acute kidney injury and poor wound healing
Design
- International, randomised controlled study
- Prior to surgery, enrolled patients were asked to complete the 12 item World Health Organisation Disability Assessment Schedule (WHODAS)
- Assignment occurred in a 1:1 ratio in permuted blocks and stratified according to site and planned postoperative destination (critical care or hospital ward) by means of a web-based service
- Most medical and nursing staff caring for patients were not blinded and had knowledge of the group assignments
- All research staff members who were responsible for the primary outcome remained blinded and unaware of group assignments
- Modified intention to treat analyses
- Only those randomised and underwent induction of anaesthesia were included in analysis
- A target of 2800 patients was initially defined
- Based upon an expected disability-free survival at 1 year of 65%
- Type I error of 0.05 and power of 90% to detect a hazard ratio of 0.80 using the log-rank test
- Included additional 5.7% to account for withdrawals and loss to follow-up
- The sample size was increased to 3000 after 2578 patients were randomised because of a greater than expected disability-free survival rate at 1 year
- This provided a final power of 80% to detect a hazard ratio of 0.78
Setting
- 47 centres in seven countries
- The mean number of patients per site was 64 (range: 1 to 227)
- May 2013 – Sept 2016
Population
- Inclusion: Adults (≥18 years) undergoing elective major surgery
- Included a skin incision, an expected operative duration of at least 2 hours, and an expected hospital stay of at least 3 days
- Who had an increased risk of post operative complications:
- defined as at least one of the following:
- age ≥70 years, the presence of heart disease, diabetes, renal impairment (>200 mmol/L (>2.8 mg/dl)), or morbid obesity (BMI ≥35 kg/m2), preoperative serum albumin <30 g/L, anaerobic threshold (if done) <12 mL/kg/min
- or two or more of the following:
- ASA 3 or 4, chronic respiratory disease, obesity (BMI 30-35 kg/m2), aortic or peripheral vascular disease, preoperative haemoglobin <100 g/L, preoperative serum creatinine 150-199 mmol/L (>1.7 mg/dl), anaerobic threshold (if done) 12-14 mL/kg/min
- Exclusion: patients undergoing urgent or time-critical surgery, liver resection, or less extensive surgery (e.g. laparoscopic cholecystectomy) or if they had end-stage kidney failure requiring dialysis
- 5223 met eligibility criteria after screening; 3000 patients were randomised
- The mean age was 66 years
- 43% underwent colorectal surgery
- 64% underwent cancer surgery
- There were no significant differences between the groups at baseline
Intervention
- Restrictive fluids
- Designed to provide a net zero fluid balance
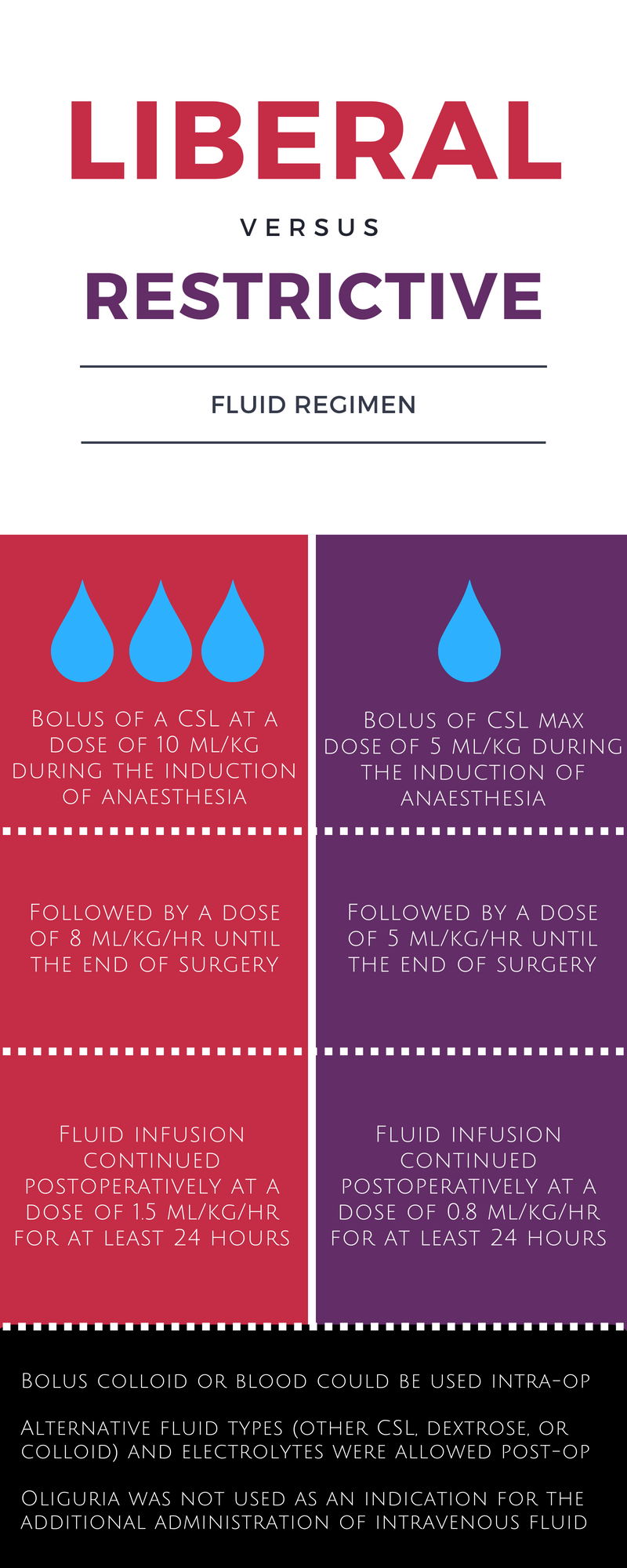
- Bolus of balanced salt crystalloid (CSL) was administered at a maximum dose of 5 ml/kg of body weight during the induction of anaesthesia
- No other intravenous fluids were to be administered before surgery unless indicated if using a goal-directed device (oesophageal Doppler or pulse wave analyser)
- This was followed by a dose of 5 ml/kg/hr until the end of surgery
- Fluid infusion was continued postoperatively at a dose of 0.8 ml/kg/hr for at least 24 hours
- The rate of postoperative fluid replacement could be reduced if there was evidence of fluid overload and no hypotension, or increased if there was evidence of hypovolemia or hypotension
- Vasopressors could first be considered for treating hypotension without evidence of hypovolemia
- The total administration of fluid during the first 24-hour period was expected to be approximately half that in the liberal fluid group
- Patients in this group received a median of 3.7 litres of fluid intravenously
Control
- Liberal fluids
- Bolus of a CSL solution was administered at a dose of 10 ml/kg of body weight during the induction of anaesthesia
- This was followed by a dose of 8ml/kg/hr until the end of surgery
- The peri-operative dose could be further reduced after 4 hours if clinically indicated
- For patients with a body weight of >100 kg, fluid volumes were calculated on the basis of a maximal body weight of 100 kg
- Fluid infusion was continued postoperatively at a dose of 1.5ml/kg/hr for at least 24 hours
- This dose could be reduced if there was evidence of fluid overload and no hypotension, or increased if there was evidence of hypovolemia or hypotension
- Patients in this group received a median of 6 litres of fluid intravenously
Management common to both groups
- Bolus colloid or blood could be used intra-operatively in the two groups to replace blood loss
- Alternative fluid types (other crystalloid, dextrose, or colloid) and electrolytes were allowed postoperatively to account for local preferences and blood biochemical findings
- Oliguria was not used as an indication for the additional administration of intravenous fluid
- All other peri-operative care was performed according to the discretion and practices of local clinicians
Outcome
- Primary outcome: No difference in disability-free survival up to 1 year after surgery
- Restrictive fluid group: 1223 patients (81.9%)
- Liberal fluid group: 1232 patients (82.3%)
- Hazard ratio for death or disability: 1.05 (95% CI 0.88 to 1.24; P=0.61)
- Disability defined as a persistent impairment in health status (lasting ≥6 months), as measured by a score of at least 24 points on the WHODAS questionnaire, which reflects a disability level of at least 25% (the threshold point between “disabled” and “not disabled”)
- Secondary outcome:
- Acute kidney injury at 30 days occurred more commonly in the restrictive fluid group
- Restrictive fluid group: 124 patients (8.6%)
- Liberal fluid group: 72 patients (5.0%)
- Risk Ratio (RR): 1.71 (95% CI 1.29 to 2.27; P < 0.001)
- Absolute Risk Increase (ARI): 3.59% (95% CI 1.76% to 5.42%; P < 0.001)
- Number needed to harm (NNH): 28
- Acute kidney injury defined according to the criteria of the Kidney Disease: Improving Global Outcomes group, on a scale of 1 to 3, with higher values indicating increased severity
- Renal-replacement therapy at 90 days occurred more frequently in the restrictive fluid therapy group, however this did not reach statistical significance after adjustment for multiple analyses
- Restrictive fluid group 0.9% vs Liberal fluid group 0.3%
- Risk Ratio: 3.27 (95% CI 1.01 to 13.8; P = 0.048)
- Threshold to reject null hypothesis was P = 0.004
- Surgical site infection occured more frequently in the restrictive fluid group, but this again was not significant after appropriate adjustment
- Restrictive fluid group 16.5% vs Liberal fluid group 13.6%
- Risk Ratio: 1.22 (95% CI 1.03 to 1.45; P = 0.02)
- Threshold to reject null hypothesis was P = 0.003
- No difference in composite of 30 day mortality or major septic complications (sepsis, surgical-site infection, anastomotic leak, or pneumonia
- Restrictive fluid group 21.8% vs Liberal fluid group 19.8%
- Risk Ratio: 1.10 (95% CI 0.96 to 1.26; P = 0.19)
- No statistically significant difference between restrictive and liberal groups, for the following:
- Median peak serum lactate levels: 1.6 vs 1.6 mmol/l
- Median peak c-reactive protein on day 3: 136 vs 133 mg/l
- Median duration of days in the intensive care unit (ICU) and hospital: 1.8 vs 1.4
- Unplanned admission to the ICU: 10.8% vs 9.7%
- Median score on quality of recovery scale: 106 vs 107
- Death at 90 days: 2.1% vs 1.2%
- Death at 12 months: 6.5% vs 6.6%
- Acute kidney injury at 30 days occurred more commonly in the restrictive fluid group
Authors’ Conclusions
- Among patients at increased risk for complications during elective major abdominal surgery, a restrictive fluid regimen was not associated with a higher rate of disability-free survival than a liberal fluid regimen and was associated with a higher rate of acute kidney injury
Strengths
- Important research question based upon a reasonable theory
- Large, multicentre, international study
- Appropriate randomised controlled trial (RCT) methodology for the hypothesis
- Adequately powered for proposed statistical analysis, which increases the strength of the conclusion and reduces the chance of false positive or false negative conclusions
- Chosen outcome is meaningful to patients
- Statistical methods are appropriate
- The use of time-based hazard ratios (‘how long until an event occurs’) increases the power of the analysis (the ability to accurately reject the null hypothesis) compared to event-based risk ratios (‘did an event occur’)
- Multiple imputed data sets allows for analysis where some data were missing without loss of power (this was used for the Acute Kidney Injury secondary outcome, where not every patient had a creatinine measured at the correct time frame)
- Holm-Bonferroni method was applied to control for multiple testing
- This adjusts the P value threshold at which an outcome is ‘significant’ when multiple hypotheses are tested on the same dataset
- The probability of a false positive (that is, rejecting the null hypothesis when we shouldn’t) remains low in exchange for a higher chance of a false negative (that is, not rejecting the null hypothesis when we should)
- Appropriate concealment of allocation sequence through the use of a web-based randomisation system
- Blinding of outcome assessors reduces the possibility of assessment bias, which would usually favour the experimental intervention group
- Pragmatic design, allowing clinicians to apply real-world decisions, which increases the external validity (generalisability)
- 1 year follow up
Weaknesses
- Although the theory is reasonable (too much or too little fluid may be harmful), the hypothesis perhaps lacks biological plausibility (can administration of either 3l or 6l in one day modify survival or disability at up to a year later?)
- Not blinded, so clinical staff may have introduced systematic biases in favour of one group or the other
- Usually this favours the experimental arm but since no difference was found there is unlikely to be significant bias from this in this trial
- Fluid administration after 24 hours of surgery was not controlled
- Many patients were not weighed on days 1-3
- Although missing data can be managed through multiple imputed datasets, it’s not as good as complete data
- Protocol amendment
- With 2,578 enrolled patients there were 300 events (disability or death) giving a 12 month event rate of 14.6%. As this was lower than expected, an increase in the trial sample size to 3,000 (≈380 events) was required to provides 80% power to detect HR≤0.75
- This protocol amendment was accepted by the Steering Committee
The Bottom Line
- In patients at increased risk for complications while undergoing elective major abdominal surgery, a restrictive fluid regimen was not associated with a higher rate of disability-free survival than a liberal fluid regimen 1 year after surgery
- However, the restrictive regimen was associated with a higher rate of acute kidney injury
- A modestly liberal fluid regimen is perhaps preferred and the goldilocks principle is reinforced – not too much, not too little, but an amount that’s just right
External Links
- [article] Restrictive versus Liberal Fluid Therapy for Major Abdominal Surgery
- [editorial] Finding the right balance
- [podcast] TopMedTalk – Monty Mython interviews Paul Myles (click below)
Metadata
Summary author: Steve Mathieu
Summary date: 16th May 2018
Peer-review editor: Duncan Chambler



Fascinating trial. No clear answer though. For comparison, in my region Harris et al conducted a multicentre audit and found that we are administering ~30ml/kg during major surgical cases, with a wide variance. RELIEF didn’t index fluid administration by weight, but roughly this puts my region’s usual practice more in line with the liberal group in this trial. Our casemix is mostly laparoscopic too.
Pingback: LITFL Review 332 | Edwin M. Thames
Working at a regional Queensland Hospital, we enrolled about 10 patients in this trial before pulling out. Almost all anesthetists objected to the set regime: the Liberal was far more fluid than they would normally give, and the restricted was far too restricted. Some of our Liberal patients developed pulmonary oedema, which is not reported on here.
so the bottom line is, lots of money was spent on a study that was counter intuitive to good clinical practice:The study compared non-standard clinical extremes of fluid intake, so it is not surprising that their Primary and secondary outcomes are largely statistically non significant. In addition to the huge cost of supporting this study, human lives and health were at risk.. The Liberal fluid intakers developed pul oedema while restricted fluid intakes had a higher risk for acute kidney injury.
We need to rethink our study designs and patient risks, prior to embarking on expensive studies.
“The study compared non-standard clinical extremes of fluid intake, so it is not surprising that their Primary and secondary outcomes are largely statistically non significant”
I would have said the opposite, they used almost absurd extremes of liberal vs restrictive regimes so you would think if there was a genuine risk or benefit of one over the other such extremes in each arm would demonstrate it, in the end almost none of the secondary outcomes reached significance, there was a slight increase in biochemically detected AKI’s but no difference in need for CRRT. The conclusion is almost absurdly obvious, too little is too little and too much is too much, somewhere in the middle is just right so use some sort of goal directed therapy to target euvoleamia and avoid excessively restrictive or liberal regimens
Mike Keane’s critique of the RELIEF study: https://trends.hms.harvard.edu/2019/02/21/do-large-clinical-trials-adequately-consider-individual-patient-physiology-debating-the-relief-study/