Drakulovic
Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomised trial
Drakulovic. Lancet 1999;354:1851-58
Clinical Question
- In patients who are mechanically ventilated does the semi-recumbent position vs. supine position reduce clinically suspected pneumonia?
Design
- Randomised controlled trial
- Computer-generated list
- Consecutive patients
- Sample size calculation: 182 patients required to show a 20% absolute risk reduction with a projected frequency in the supine group of 40%, with a false negative rate of 20% and false positive rate of 5%
- Planned interim analysis completed after 50% recruitment. This demonstrated a significant difference and the trial was stopped early
- Modified intention to treat analysis
- Non-blinded
- Univariate and multivariate analysis completed
Setting
- A respiratory ICU and a medical ICU in a tertiary university hospital in Spain
- June 1997 – May 1998
Population
- Inclusion criteria: Not stated
- Exclusion criteria: Abdominal or neurosurgical intervention within 7 days; shock refractory to vasoactive drugs or volume therapy; previous endotracheal intubation within 30 days
- 90 patients randomised
- 47 patients randomised to control group, all completed and included in trial
- 43 patients randomised to intervention group, 4 patients excluded (1 died during resuscitation, 3 excluded due to protocol violation [re-intubation])
- Comparing intervention vs. control groups
- Mean age: 67 vs. 63
- Cause of acute respiratory failure
- COPD: 34% vs. 33%
- Other pulmonary diseases 26% vs. 21%
- Mean APACHE II Score: 23.8 vs. 21.3
- Duration of mechanical ventilation (hrs): 171 vs. 145
- Use of large bore NG tube: 87% vs. 72%
- Enteral nutrition: 60% vs. 56%
Intervention
- Semi-recumbent (45 degrees)
Control
- Supine body position (0 degrees)
All patients routinely subjected to:
- Sterile endotracheal suctioning
- No change of mechanical ventilation tubing systems
- Stress ulcer prophylaxis with sucralfate in patients who tolerated enteral nutrition, and IV ranitidine or omperazole in patients receiving TPN
- Enteral nutrition
- Starting rate 33.3ml/hr
- Gastric aspiration performed every 4 hours
- Target feed 30-35 kcal/kg/day
Study completed when any of the following criteria met:
- 1st weaning trial
- Extubation
- Permanent change in body position for >45 minutes
- Death
Outcome
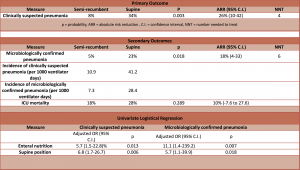
- Primary outcome: frequency of clinically suspected pneumonia (Defined as new and persistent infiltrates on Chest x-ray most likely to be due to infection, + at least 2 of: temp >38.3; WBC <4 or >12; purulent tracheal secretions)
- Significantly lower in semi-recumbent vs. supine: 8% vs. 34% (95% C.I. for difference 10-42, P=0.003)
- Secondary outcomes:
- Microbiological confirmed pneumonia (defined in patient with clinically suspected pneumonia with bacterial growth above defined threshold of pathogenic microorganism in tracheobronchial aspirate, bronchoalveolar lavage, or protected specimen brush)
- Significantly lower in semi-recumbent vs. supine: 5% vs. 23% (95% C.I. for difference 4-33, P=0.018)
- Incidence rate of microbiologically confirmed pneumonia 7.3/1000 ventilator days in semi-recumbent vs. 28.4/1000 ventilator days in supine
- Incidence of clinically suspected pneumonia: 10.9/1000 ventilator days in semi-recumbent vs. 41.2/1000 ventilator days in supine
- ICU mortality – no significant difference
- 18% in semi-recumbent vs. 28% in supine (95% C.I. -7.6 to 27.6, P=0.289)
- Univariate logistic regression analysis demonstrated that enteral nutrition and supine body position were significantly associated with clinically suspected and microbiologically confirmed pneumonia
- Microbiological confirmed pneumonia (defined in patient with clinically suspected pneumonia with bacterial growth above defined threshold of pathogenic microorganism in tracheobronchial aspirate, bronchoalveolar lavage, or protected specimen brush)
Authors’ Conclusions
- In mechanically ventilated patients nosocomial pneumonia is reduced with the use of a semi-recumbent position
Strengths
- Randomised controlled trial
- Clear definition for primary and secondary outcomes
Weaknesses
- Terminated early with low number of patients included
- Outcome assessors non-blinded
- Inclusion criteria not clearly defined
- Single hospital
The Bottom Line
- This small randomised trial has a number of weaknesses, but still provides convincing evidence that the risk of clinically suspected, and microbiologically confirmed pneumonia, is reduced in mechanically ventilated patients who are semi-recumbent vs. supine.
External Links
- [article] Supine body position as a risk factor for nosocomial pneumonia in mechanically ventilated patients: a randomised trial
- [further reading] PulmCCM: Ventilator bundles (VAP bundles) not evidence-based, shouldn’t be standard care
- [Further reading] Preventing Ventilator-Associated Pneumonia Does the Evidence Support the Practice?
- [Further reading] Critical Care Network in North West London: Ventilator Care Bundle
Metadata
Summary author: Dave Slessor
Summary date: 6th December 2015
Peer-review editor: Steve Mathieu


