Monnet
Passive leg-raising and end-expiratory occlusion tests perform better than pulse pressure variation in patients with low respiratory system compliance
Monnet. Critical Care Med. 2012; 40:152-157
Clinical Question
- In patients who are mechanically ventilated, does the tidal volumes or compliance, affect the performance of pulse pressure variation to predict volume responsiveness? In addition, in patients with ARDS can a passive leg raise test or end-expiratory occlusion test predict fluid responsiveness?
Design
- Prospective observational study
- Blinding not stated
- Use of consecutive patients not stated
- Statistics
- Data pre + post fluid challenge compared using paired Student t test or Wilcoxon paired test, as appropriate
- Comparison of data between different groups performed using two-sample Student t test or a Mann-Whitney U test, as appropriate
- Comparison of ROC curves tested with Hanley-McNeil test
Setting
- Single medical ICU, Paris
- Dates of data collection not stated
Population
- Inclusion criteria: Mechanically ventilated patients with circulatory failure who required a fluid challenge
- Circulatory failure:
- BP ≤90mmHg (or decrease of ≥50 in known hypertensive)
- And at least 1 of the following
- Urinary flow ≤0.5ml/kg/min for ≥2 hours
- HR ≥100
- Skin mottling
- Need for fluid challenge as determined by attending physician
- Mechanical ventilation in assist control mode
- Absence of cardiac arrhythmias and spontaneous triggering of ventilator, as assessed by 2 investigators using airway pressure curve
- Circulatory failure:
- Exclusion criteria:
- <18 years
- Moribund
- Passive leg raise contraindicated (head trauma, venous compression stocking)
- All patients sedated, and 5 patients paralysed
- 54 patient included
- 44 septic patients
- 27 patients had ARDS, Compliance was 22ml/cmH20 in these patients
- 27 patients did not have ARDS, Compliance was 45ml/cmH2O in these patients
Tests of Interest
- Pulse pressure variation (PPV)
- Measured pre and post-fluid challenge
- Passive leg raise (PLR)
- Patient transferred from 45° semirecumbent position to supine with legs raised to 45°
- Cardiac output studies recorded when changes induced by PLR were maximal i.e. within 1 minute
- End-expiratory occlusion (EEO)
- End-expiratory hold for 15 seconds
- Cardiac output studies recorded at end of EEO
For both PLR and EEO, baseline cardiac output measurements performed at baseline and 1 minute post test of interest.
Gold Standard Investigation
- Fluid challenge
- Following PLR and EEO tests, patient given 500ml normal saline over 20 minutes
In all patients cardiac output studies performed using a PiCCO2 device. Measurements taken at baseline, post-test of interests and post-fluid challenge. Volume responder defined as increase in Cardiac index (CI) ≥15%
Outcome
- Volume responders
- Fluid challenge significantly increased CI ≥15% (+44% ±39%) in 30 ‘volume responders’
- In patients with ARDS there were 16 responders and 11 non-responders
- In patients without ARDS there were 14 responders and 13 non-responders
- Primary outcome: Pulse pressure variation
- Significantly correlated with compliance (r=0.55, p=0.0001)
- Not correlated with tidal volume (r=0.21, p=0.13)
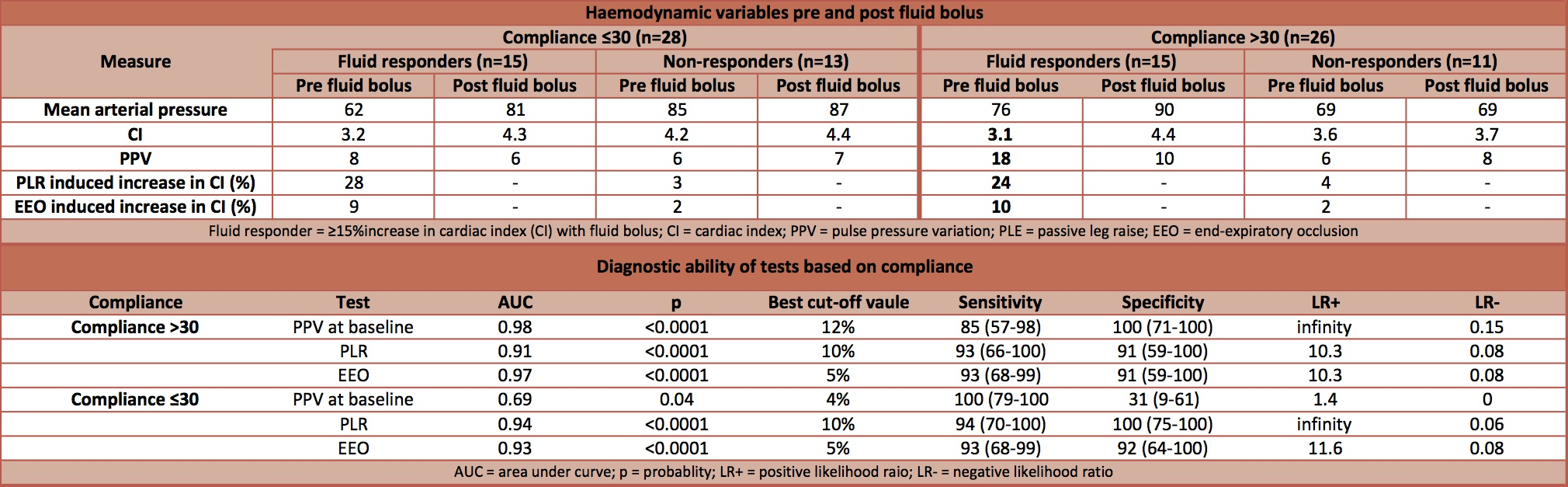
- Significantly higher in volume responders with compliance >30ml/cmH20 vs. ≤30ml/cmH20 (18% vs. 8%). Whereas in non-responders there was no significant difference
- All patients that had a PPV of >12% were found to be fluid responsive regardless of the compliance. The poor performance at predicting fluid responsiveness in patients with a low compliance was due to the false negative results.
Passive Leg Raise
- Changes in CI induced by PLR not significantly correlated with compliance (r=-0.09) or with tidal volume (r=0.14)
- Significant increase in CI induced by PLR in volume responders with both low and high compliance (28% and 24% respectively)
- In non-volume responders no significant increase in CI with PLR
End-expiratory occlusion
- Changes in CI induced by EEO signficantly correleated with compliance
- Significant increase in CI induced by EEO in volume responders with both low and high compliance (9% and 10% respectively)
- In non-volume responders no significant increase in CI with EEO
Authors’ Conclusions
- Pulse pressure variation is less accurate at predicting fluid responsiveness in patients with low compliance, but passive leg raising and End-Expiratory Occlusion test remain valuable in these circumstances.
Strengths
- Clear inclusion and exclusion criteria
- Analysed for effects of both tidal volume and compliance
- 3 tests of interest compared with results from fluid challenge
Weaknesses
- Not stated if consecutive patients enrolled
- No sample size calculation
- Single centre
- Authors on advisory board of Pulsion Medical Systems
The Bottom Line
- Pulse pressure variation performed poorly at predicting fluid responsiveness in patients with a low compliance, irrespective of lung volumes. This was due to to a high false negative rate.
- Increases in cardiac index induced by passive leg raising and end-expiratory occlusion performed well at predicting fluid responsiveness in patients with both a high and low compliance.
External Links
- [article] Passive leg-raising and end-expiratory occlusion tests perform better than pulse pressure variation in patients with low respiratory compliance
- [podcast] EMCrit: fluid responsiveness
- [SMACC podcast via EmCrit] Rob MacSweeney vs Paul Marik – Predicting Fluid Responsiveness is a Waste of Time
- [further reading] Will this haemodynamically unstable patient respond to a bolus of intravenous fluids?
- [further reading] Predicting Fluid Responsiveness in Critically Ill Patients by Using Combined End-Expiratory and End-Inspiratory Occlusions With Echocardiography
Metadata
Summary author: @davidslessor
Summary date: 27th April 2016
Peer-review editor: @avkwong



Pingback: LITFL Review 230 | LITFL: Life in the Fast Lane Medical Blog