POCUS: Batllori
Randomized comparison of three transducer orientation approaches for ultrasound guided internal jugular venous cannulation
Batllori et al. BJA 2015 doi: 10.1093/BJA/aev399
Clinical Question
- In patients undergoing internal jugular cannulation under ultrasound guidance, does the use of an oblique compared to short- and long-axis approach increase success rate and decrease complications?
Design
- Single centre, prospective, randomised study
- Unblinded
- Randomisation by computer-generated number list
- Followed up until catheter removed with all tips sent for culture
- Power calculation based on assumption of 60% first needle pass cannulation in Short Axis (SAX) group and to detect a 20% difference between the groups
- alpha-level 0.05, 80% power
- 70 patients per group required
- Intention-to-treat analysis
Setting
- Single hospital in Spain
- April 2012 – March 2013
Population
- Inclusion:
- 18 years and above
- Indication for IJV cannulation
- Exclusion:
- <18 years
- History of previous surgical intervention at the cannulation site
- Presence of a CVC during the past 72 hours (in the same vein as the cannulation was planned)
- Infection, haematoma or surgical emphysema close to the puncture site
- Recent cervical trauma with present neck immobilisation
- Altered haemostasis (INR >2, platelet count < 50,000)
- Agitated or uncooperative patient
- Cannulation planned to be performed outside of the surgical area
- Urgent cannulation
- 231 patients screened, 220 randomised
Common intervention
- Performed by three anaesthetists
- Structured training programme: 2 hour lecture, 1 hour beside teaching, 1 hour supervised practice using phantom
- Previously had 10 successful cannulations in each of the three views
- Linear array probe
- Performed either in theatre or post-anaesthetic care unit
- Full asepsis.
- Real-time ultrasound guidance
- Seldinger technique for CVC insertion
- Chest radiograph performed to assess position of catheter and presence of complications
Short-axis (SAX)
- Probe placed transversely over neck
- Needle introduced in a plane perpendicular to long-axis of transducer
Long-axis (LAX)
- Probe place longitudinally over neck
- Needle introduced underneath footprint of probe following its long axis
Oblique-axis (OAX)
- SAX first obtained
- Probe rotated to a position midway between SAX and LAX view
- Needle introduced underneath footprint of probe aiming from lateral to medial
Outcome
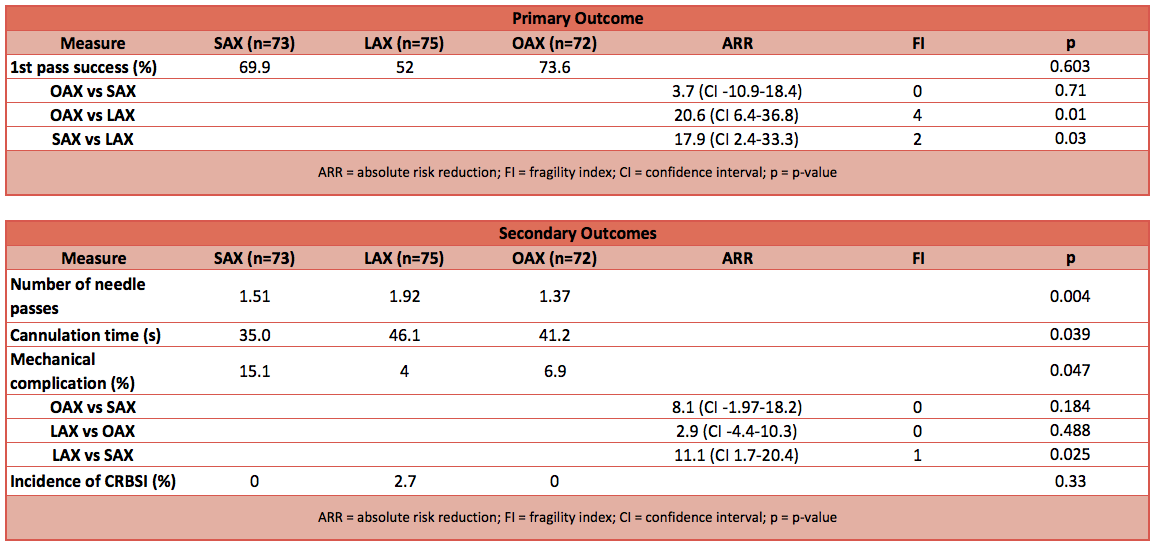
- Primary outcome:
- First needle pass cannulation rate (needle pass was considered as any forward movement of needle without any backward movement, irrespective of skin puncture)
- Higher 1st pass success rate in OAX vs LAX (OR 3.7, CI 1.71-8)
- Higher 1st pass success rate in SAX vs LAX (OR 2.37, CI 1.16-4.86)
- No difference between OAX and SAX
- First needle pass cannulation rate (needle pass was considered as any forward movement of needle without any backward movement, irrespective of skin puncture)
- Secondary outcome:
- Number of needle passes until successful cannulation
- More needle passes required in LAX vs OAX
- More needle passes required in LAX vs SAX
- No difference between OAX and SAX
- Cannulation time measured in seconds
- Longer cannulation time in LAX vs SAX
- Incidence of mechanical complications (including arterial puncture, posterior wall puncture, pneumothorax and haemothorax)
- Higher complication rate in SAX compared to LAX and OAX
- Commonest complication was puncture through the posterior wall
- Incidence of catheter-related bloodstream infection
- 2 in LAX group but not statistically significant
- Number of needle passes until successful cannulation
Authors’ Conclusions
- OAX and SAX are better than LAX in terms of cannulation quality outcomes and that OAX is a safe and effective approach to performing IJV cannulation and should be encouraged
Strengths
- Comprehensive training programme for operator
- Clear definition of what constitutes a needle pass
- Analysis between operators
Weaknesses
- Small number of operators already experienced and accredited in ultrasound-guided IJV cannulation
- Elective setting
- Vast majority of insertions (87%) performed in anaesthetised patients
The Bottom Line
- This study confirms the view that ultrasound-guided IJV cannulation is quicker and technically less demanding in SAX compared to LAX but is associated with greater risk of complication. OAX is a relatively less well-known approach which has the potential to combine the advantages of SAX and LAX but requires further evaluation and training.
External Links
- [article] Randomized comparison of three transducer orientation approaches for ultrasound guided internal jugular venous cannulation
- [further reading] AAGBI Safer Vascular Access 2016
- [further reading] The oblique view: an alternative approach for ultrasound-guided central line placement
Metadata
Summary author: Adrian Wong
Summary date: 26 October 2016
Peer-review editor: Duncan Chambler


