INPRESS

Effect of Individualized vs Standard Blood Pressure Management Strategies on Postoperative Organ Dysfunction Among High-Risk Patients Undergoing Major Surgery
Futier E et al. JAMA 2017; doi:10.1001/jama.2017.14172
Clinical Question
- In high-risk patients undergoing surgical procedures, does a strategy of targeting individualised systolic blood pressure compared to standard practice reduce organ dysfunction?
Background
- The number of patients undergoing surgical procedures worldwide is growing
- More recent trials of early goal-directed therapy pathways have not been shown to be superior to standard therapy
- SEPSISPAM trial found no mortality difference in patients with septic shock who underwent resuscitation targeting a mean BP of either 65 to 70mmHg or 80 to 85mmHg
Design
- Multicenter, stratified, parallel-group, randomised controlled trial
- 1:1 ratio to controlled and intervention group
- Randomisation using minimisation algorithm and stratified according to study site, urgency or surgery and surgical site
- Sample size of 268 patients for 90% power to detect an absolute difference of 20% in primary outcome, a 2-sided α-level of 0.05, assuming an event rate of 40% in control arm
- Recruitment target of 300 to account for potential protocol deviations and withdrawal of consent
- Intention to treat analysis
- Intervention could not be blinded but attempts to reduce bias by online randomisation to ensure concealment of group assignment and blinding post-op carers
Setting
- 9 university and non-university hospitals in France
- December 2012 – August 2016
Population
- Inclusion:
- Aged above 50
- Undergoing surgery under general anaesthesia with an expected duration of more than 2 hours
- American Society of Anesthesiology score of 2 or higher
- Preoperative Acute Kidney Injury Risk Index of class 3 or higher
- Exclusion:
- Uncontrolled hypertension (systolic BP > 180mmHg or diastolic BP > 110mmHg)
- Chronic kidney disease (GFR < 30ml/min/1.73m2 or requiring renal replacement therapy)
- Acute or decompensated heart failure
- Acute coronary syndrome
- Preoperative sepsis
- Already receiving norepinephrine infusion
- Pregnant or breastfeeding
- 1494 patients screened, 298 randomised; 149 in each arm
- Baseline characteristics similar with 84% of procedures being elective procedures and the vast majority of surgery in both groups involving the abdomen (93.9% and 96.6%). Significant proportion of patients in both groups had pre-existing chronic arterial hypertension (82%)
Intervention
- Continuous infusion of norepinephrine used to target a systolic blood pressure (SBP) within 10% of reference value
- Infusion rate reduced if heart rate < 40 bpm
Control
- Intravenous ephedrine at 6 mg boluses (up to 60mg) administered as recommended for SBP < 80 mmHg or if 40% lower than reference value
- If SBP remained below target after maximum dose of 60mg ephedrine administered, norepinephrine permitted as rescue therapy
Management common to both groups
- Resting blood pressure from preoperative assessment used as reference value; if not available, the blood pressure was measured on the surgical ward, the day before surgery
- Invasive blood pressure measurement through a radial catheter required
- Ringers Lactate solution infused at 4ml/kg/hr as maintenance fluid
- Additional fluid were given based on a protocolised haemodynamic algorithm (stroke volume index optimisation) using 6% hydroxyethyl starch solution in 250ml boluses
- Intervention period lasted from anaesthetic induction to 4 hours after the completion of surgery
- Decisions regarding all other aspects of care was left at the discretion of the attending physician
Outcome
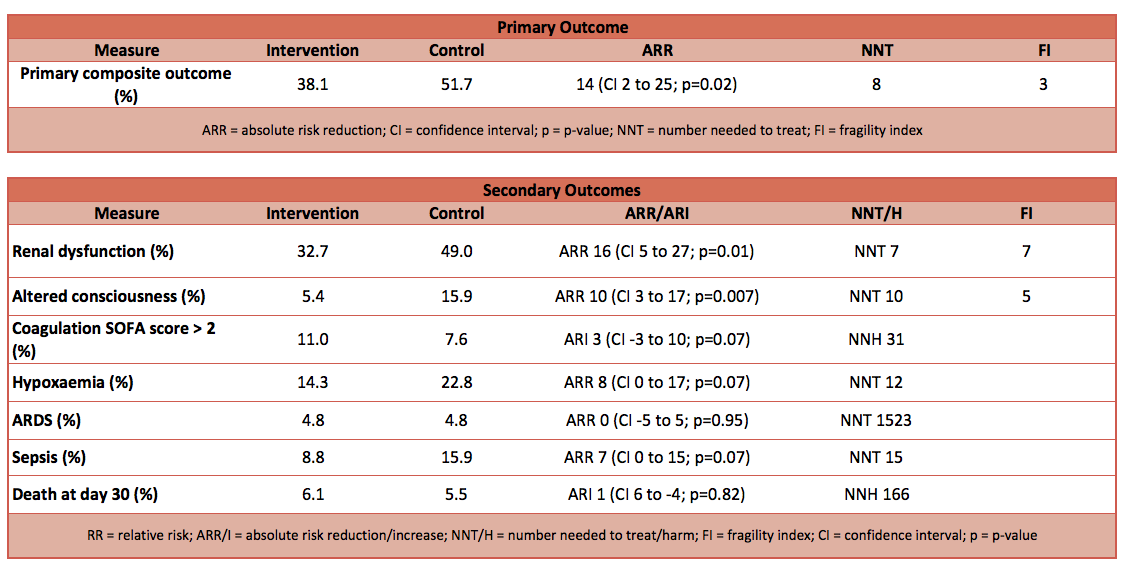
- Primary outcome: Composite of systemic inflammatory response syndrome (SIRS) and at least 1 organ system dysfunction for renal, respiratory, cardiovascular, neurological and coagulation system occurring by day 7 after surgery – Lower event rate in intervention group
- 38.1% in intervention group compared to 51.7% in control
- Absolute risk reduction (ARR): 14% (95% CI -25% to -2%; P = 0.02)
- Number needed to treat (NNT): 8
- Fragility index (FI): 3
- Secondary outcome: Individual components of the primary outcome and adverse events
- Renal dysfunction lower:
- Intervention group 32.7% vs Control 49.0%
- ARR: 16% (95% CI -27% to -5%; P = 0.01)
- NNT: 7
- FI: 7
- Altered consciousness lower:
- Intervention group 5.4% vs Control 15.9%
- ARR: 10% (95% CI -17% to -3%; P = 0.007)
- NNT: 10
- FI: 5
- No significant difference in:
- SIRS score
- Coagulation SOFA score
- Hypoxaemia
- Pneumonia
- ARDS
- Reintubation rates
- SOFA scores on day 1, 2 and 7
- Incidence of sepsis
- Surgical complications
- Death at 30 days
- Renal dysfunction lower:
Authors’ Conclusions
- Management targeting an individualised systolic blood pressure, compared with standard management, reduced the risk of postoperative organ dysfunction
Strengths
- Relevant and important clinical question
- Targeted higher risk population
- Clear separation of systolic, mean and diastolic BP between groups at the end of intervention (no difference between groups pre-induction of anaesthesia)
- Although a composite score was used as primary outcome, the components are clinically relevant
Weaknesses
- Slow recruitment despite high number of patients screened
- Majority of patients were excluded due to AKI risk index of < 3
- The routine use of invasive blood pressure monitoring may not be reflective of current practice
The Bottom Line
- Targeting individualised BP reduces the rate of post-operative organ dysfunction in patients undergoing surgery
- The increased used of arterial cannulation and norepinephrine infusion does not seem to increase adverse outcomes
External Links
- [article] Effect of Individualized vs Standard Blood Pressure Management Strategies on Postoperative Organ Dysfunction Among High-Risk Patients Undergoing Major Surgery
- [further reading] Accompanying editorial
- [further reading] SEPSISPAM: High versus low Blood-Pressure Target in Patients with Septic Shock
Metadata
Summary author: Adrian Wong
Summary date: 5/10/2017
Peer-review editor: Segun Olusanya


