Ramachandran
Apneic oxygenation during prolonged laryngoscopy in obese patients: a randomized, controlled trial of nasal oxygen administration
Ramachandran. Journal of Clinical Anesthesia 2010;22:164-168. doi:10.1016/j.jclinane.2009.05.006
Clinical Question
- In obese patients with simulated difficult laryngoscopy, does the use of nasal oxygen prolong the duration that oxygen saturations remain ≥95%?
Design
- Randomised controlled trial
- Non-blinded
- Allocation concealment maintained
- Power calculation: To detect a difference of ≥60 seconds, 30 patients would be required with a
- probability of false positive trial 5%
- probability of false negative trial 20%
Setting
- Single university hospital, USA
- Dates of data collection not reported
Population
- Inclusion: elective surgery with general anaesthesia, BMI 30-35
- Exclusion: female, smoker, cardiac/respiratory disease, reflux, raised intracranial pressure, SpO2 ≤ 97% on 100% via face mask, Grade 3 or 4 mask ventilation or laryngoscopic view (current or past)
- 30 patients analysed out of 33 randomised
Intervention
- 5L/min O2 via nasal prongs
- applied prior to pre-oxygenation and continued until post-intubation
Control
- No O2 via nasal prongs
All patients in intervention and control groups
- had standardised induction technique
- had pre-oxygenation with head up 25° and at least 8 vital capacity breaths until end-tidal O2 % was >90%
- at 60 seconds had laryngoscopy performed
- If Cormack and Lehane grade 3 or 4 then excluded from study
- If Cormack and Lehane grade 1 or 2 then force on laryngoscope blade reduced to simulate a grade 4 view. At 6 minutes, or when SpO2 decreased to 95%, tracheal intubation was performed
Outcome
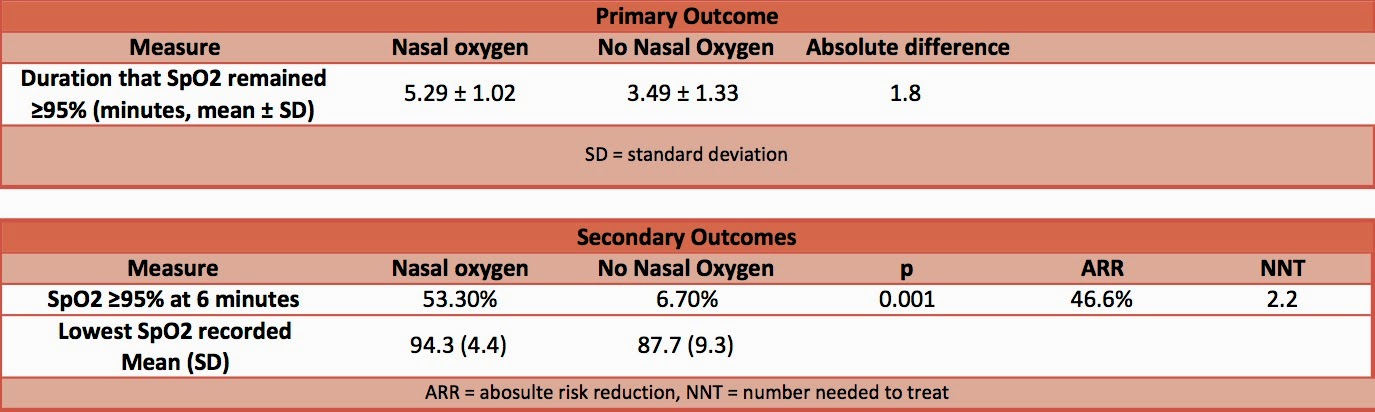
- Primary outcome:
- Patients not given nasal O2 had a significantly shorter duration of time that SpO2 was ≥95% compared to patients who received nasal oxygen
- Secondary outcomes:
- The number of patients with SpO2 ≥95% at 6 minutes was significantly greater in patients receiving nasal O2
- The lowest SpO2 recorded was significantly lower in patients who did not receive nasal O2
Authors’ Conclusions
- Nasal oxygen significantly increased the duration of SpO2 ≥95% during simulated difficult laryngoscopy in obese patients
Strengths
- Randomised
- Maintained allocation concealment
Weaknesses
- Single centre
- Small sample size
- Non-blinded
The Bottom Line
- The addition of nasal oxygen from pre-oxygenation until post-intubation significantly prolonged the duration that oxygen saturations remained ≥95% in simulated difficult airways. There are some methodological limitations, in particular the lack of blinding. However, as those treated with nasal oxygen had such significant gains and the treatment has minimal side effects, this will become my standard practice for critically ill patients. If during RSI you have an episode of hypoxia and you have not applied nasal O2 the question should be asked as to why not.
External Links
- [article abstract] Apneic oxygenation during prolonged laryngoscopy in obese patients: a randomized, controlled trial of nasal oxygen administration
- [further reading] St. Emelyns Best Bet apneic oxygenation during endotracheal intubation
- [further reading] EMCrit: Preoxygenation, Reoxygenation and Deoxygenation
- [further reading] Difficult Airway Society Proposed Guideline 2015 including the use of apneic oxygenation
Metadata
Summary author: @davidslessor
Summary date: 23rd October 2014
Peer-review editor: @stevemathieu75


