TRISS
Lower versus Higher Hemoglobin Threshold for Transfusion in Septic Shock
TRISS Trials Group. N Engl J Med 2014; 371:1381-1391. DOI: 10.1056/NEJMoa1406617
Clinical Question
- In patients with septic shock, does blood transfusion at a lower or higher haemoglobin threshold improve mortality?
Design
- Randomised controlled trial
- Stratified by study site and presence of active haematological cancer
- Permuted blocks of varying sizes
- Blinding of treatment assignments to investigators assessing primary outcome, and trial statistician
- Intention to treat analysis
- Power calculation: Assuming a mortality in the higher transfusion threshold of 45%, 1000 patients would be able to detect a 9% absolute risk reduction in mortality
- probability of
- false positive result 5%
- false negative result 20%
- probability of
Setting
- 32 general ICUs in Scandinavia
- December 2011 – December 2013
Population
- Inclusion: adult patients with septic shock and Hb≤9g/dl
- Exclusion: previous adverse reaction to transfusion, received blood transfusion in ICU, acute coronary syndrome, life threatening bleeding, acute burn, withdrew from active therapy
- Primary outcome data obtained for 998 patients out of 1005 who were randomised
- Comparing lower vs higher threshold groups – no significant difference in baseline characteristics
- surgery during index hospitalisation
- emergency 38% vs. 43.8%
- elective 11.8% vs. 10.7%
- source of sepsis
- lungs 53.2% vs. 52.2%
- abdomen 41% vs. 39.9%
- urinary tract 11.6% vs. 12.3%
- soft tissue 11.8% vs. 11.9%
- other 10% vs. 9.5%
- history of chronic cardiovascular disease 14.9% vs. 13.3%
- positive culture 37.5% vs. 32.3%
- surgery during index hospitalisation
Intervention
- Transfusion threshold of ≤7g/dl
Control
- Transfusion threshold of ≤9g/dl
In both intervention and control groups
- Patients given single unit crossmatched, prestorage leukoreduced red cells when met transfusion threshold
- Intervention period was entire ICU stay, to a maximum of 90 days after randomisation
- If life threatening bleeding, ischaemia or required ECMO then attending doctor could transfuse at haemoglobin threshold decided by doctor
Outcome
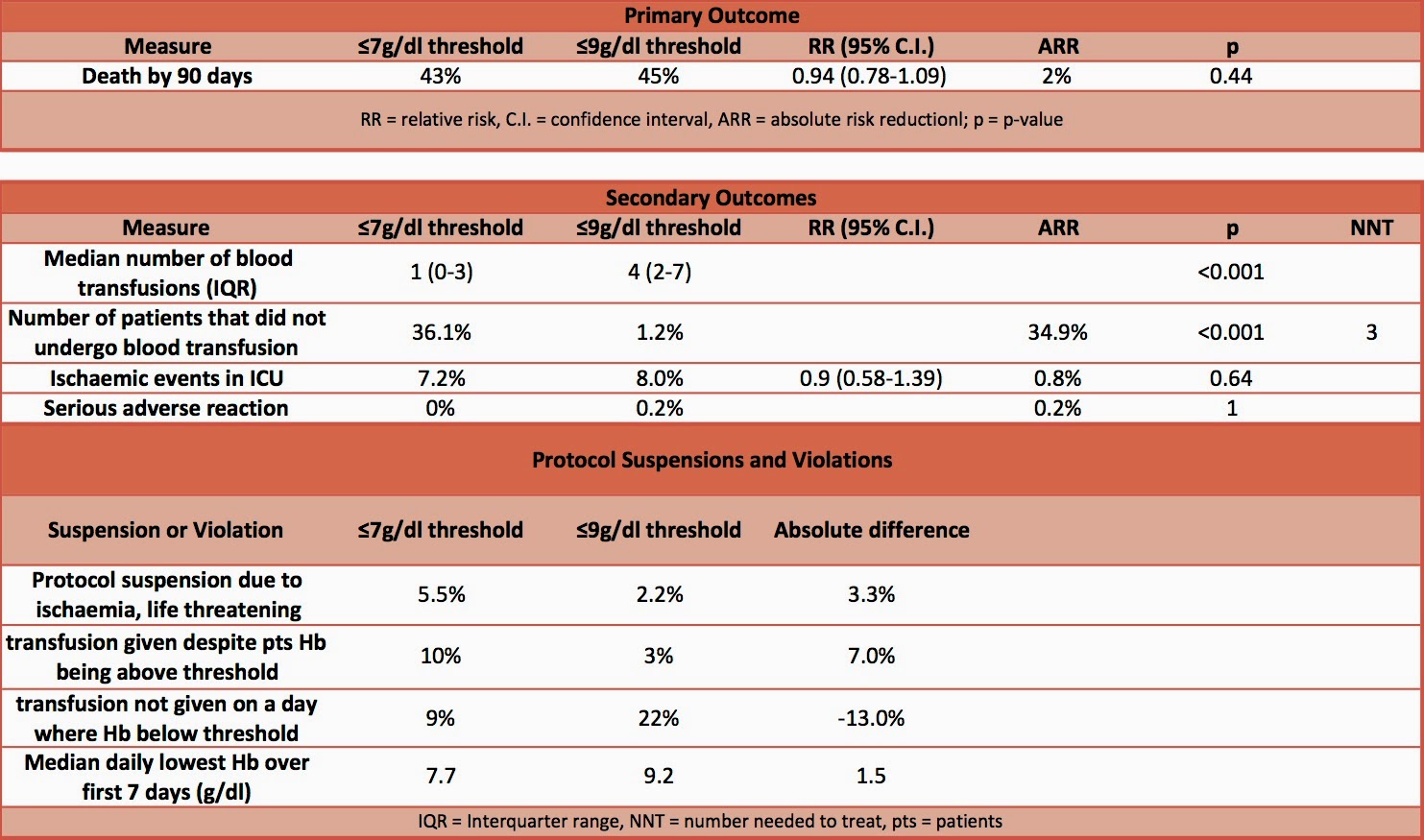
- Primary outcome: death by 90 days – no significant difference
- Secondary outcomes:
- median number of blood transfusions – significantly more in lower threshold
- number of patients that did not undergo blood transfusion – significantly less in lower threshold
- no significant difference in
- use of life support at days 5, 14, 28
- percentage of days alive without
- vasopressor/inotropic support
- mechanical ventilation
- renal replacement therapy
- percentage of days alive and out of the hospital
- complications – no significant difference
- Sub-group analysis
- no significant difference in primary outcome based on presence/absence of chronic cardiovascular disease, age > or ≤70, SAPS II of > or ≤53
- Protocol suspensions and violations
- more likely to be given transfusion as either a suspension or violation if target threshold ≤7g/dl and more likely to have transfusion withheld if target threshold ≤9g/dl
Authors’ Conclusions
- In patients with septic shock, mortality and rates of ischaemic events were similar in those assigned to a blood transfusion at a higher vs. lower threshold
Strengths
- Randomised
- Blinding of investigators assessing primary outcome
- Multi-centre
Weaknesses
- Non-blinding of staff – however this would be unrealistic to achieve
- Protocol violations mean that the study is less likely to detect a difference if there really is one. However, there was still a difference of 1.5g/dl between the daily lowest Hb levels in the intervention and the control groups. The authors also performed a per-protocol analysis which found no difference in the primary outcome.
The Bottom Line
- In patients with septic shock and managed in an ICU setting, a transfusion threshold of 7g/dl compared with 9g/dl resulted in no difference in mortality or ischaemic events. This paper supports my current practice. Avoiding unnecessary blood transfusion removes the risk of infectious, immune and non-immune related complications as well as conserving this limited resource. However, in this study 10% of patients, in the low threshold group, received transfusions despite being above the treatment threshold, therefore there may be times when the threshold needs to be modified.
- Patients with acute coronary syndromes were excluded from this trial. Further research is needed to assess the safety of lower haemoglobin thresholds for transfusion in these patients.
External Links
- [Abstract only] [Lower versus Higher Hemoglobin Threshold for Transfusion in Septic Shock]
- [Further reading] Summary of TRICC – The Bottom Line
- [Further reading] Summary of Transfusion Strategies for Acute Upper GI Bleeding – The Bottom Line
- [Videocast] ESICM Lars Holst Hot Topics Session
Metadata
Summary author: @davidslessor
Summary date: 7th October 2014
Peer-review editor: @stevemathieu75


Pingback: TRICOP – The Bottom Line
Pingback: New summary: TRICOP, Liberal Versus Restrictive Transfusion Strategy in Critically Ill Oncological Patients: The Transfusion Requirements in Critically Ill Oncologic Patients Randomized Controlled Trial – Critical Care: In The Know
Pingback: TRICS-III – The Bottom Line
Pingback: TRACT Tranfusion Timing – The Bottom Line
Pingback: REALITY – The Bottom Line
Thank you for the great comprehension!
I think there is however a small mistake in the secondary outcomes comprehension:
You wrote:
Secondary outcomes:
median number of blood transfusions – significantly more in lower threshold
number of patients that did not undergo blood transfusion – significantly less in lower threshold
if I’m not getting this entirely wrong it has to be less in the first and more in the second line. See also the Outcome Table you provided.
With kind regards from Germany, keep up the great work!
Jan B.
As the above comment: a slight error: Secondary outcomes: median number of blood transfusions – significantly more in lower threshold
it should be less.
The correct figures are that the lower-threshold group received a median of 1 unit of blood (interquartile range, 0 to 3) and the higher-threshold group received a median of 4 units (interquartile range, 2 to 7).
Cheers
Tom