The Swedish Spinal Stenosis Study

A Randomized, Controlled Trial of Fusion Surgery for Lumbar Spinal Stenosis
Forsth NEJM 2016;374:1413-23. doi:10.1056/NEJMoa1513721
Clinical Question
- In patients with lumbar spinal stenosis at 1 or 2 adjacent vertebral levels, with or without spondylolisthesis, what is the efficacy of decompression surgery compared with decompression and fusion surgery, on functional outcome assessed 2 years post-operatively?
Design
- Multi-centred, randomised, controlled trial
- Blinding of outcome assessors only
- Randomisation was stratified to the presence or absence of spondylolisthesis (forward displacement of a vertebra)
- Allocation concealment achieved by a web-based randomisation sequence
- Pragmatic design such that the surgical technique was determined by the surgeons, who were highly experienced in performing the two trial interventions
- The initial sample size was calculated assuming that the ratio of those with spondylolisthesis and those without was 1:3. However, the proportion of patients with spondylolisthesis was higher which meant that the goal of including 40 patients in each of the 4 stratum was achieved earlier than predicted. This allowed an 80% power to detect a difference in the ODI (Oswestry Disability Index) of 12 points. So following recalculation the number included in each group was more than 40 and 247 patients in total were randomised
- Per-protocol analysis, but an intention to treat analysis also conducted
Setting
- 7 Swedish hospitals
- 247 patients were enrolled between October 2006 and June 2012
Population
- Inclusion: Patients aged 50-80 years; pseudoclaudication in one or both legs and back pain; 1 or 2 adjacent stenotic segments (cross-section area of dural sac < 75mm2); Duration of symptoms > 6 months
- Exclusion: Spondylolysis (a defect or stress fracture in the pars interarticularis of the vertebral arch); degenerative lumbar scoliosis; history of lumbar spinal surgery for stenosis or instability; stenosis not due to degenerative changes; stenosis caused by a herniated disk; other specific spinal conditions (e.g cancer, ankylosing spondylitis); history of vertebral fractures in affected segments; psychological disorders (e.g dementia, drug abuse)
- 247 patients
Intervention
- Fusion Group = decompression and fusion
Control
- Decompression alone group
Outcome
- Primary outcome: per protocol analysis of Oswestry Disability Index (ODI) at 2 years.
- no difference between the groups in the mean ODI
- 27 in the fusion group vs 24 in decompression alone group, P=0.24
- no statistical difference in the change of ODI
- decrease from baseline of 15 in the fusion group and 17 in the decompression alone group, P = 0.36
- no significant difference in outcome between type of treatment and the presence or not of spondylolithesis
- no difference between the groups in the mean ODI
ODI is a standard scoring system which measures the degree of disability and quality of life in patients with lower back pain. This score ranges from 0-100, with higher scores indicating more severe disability
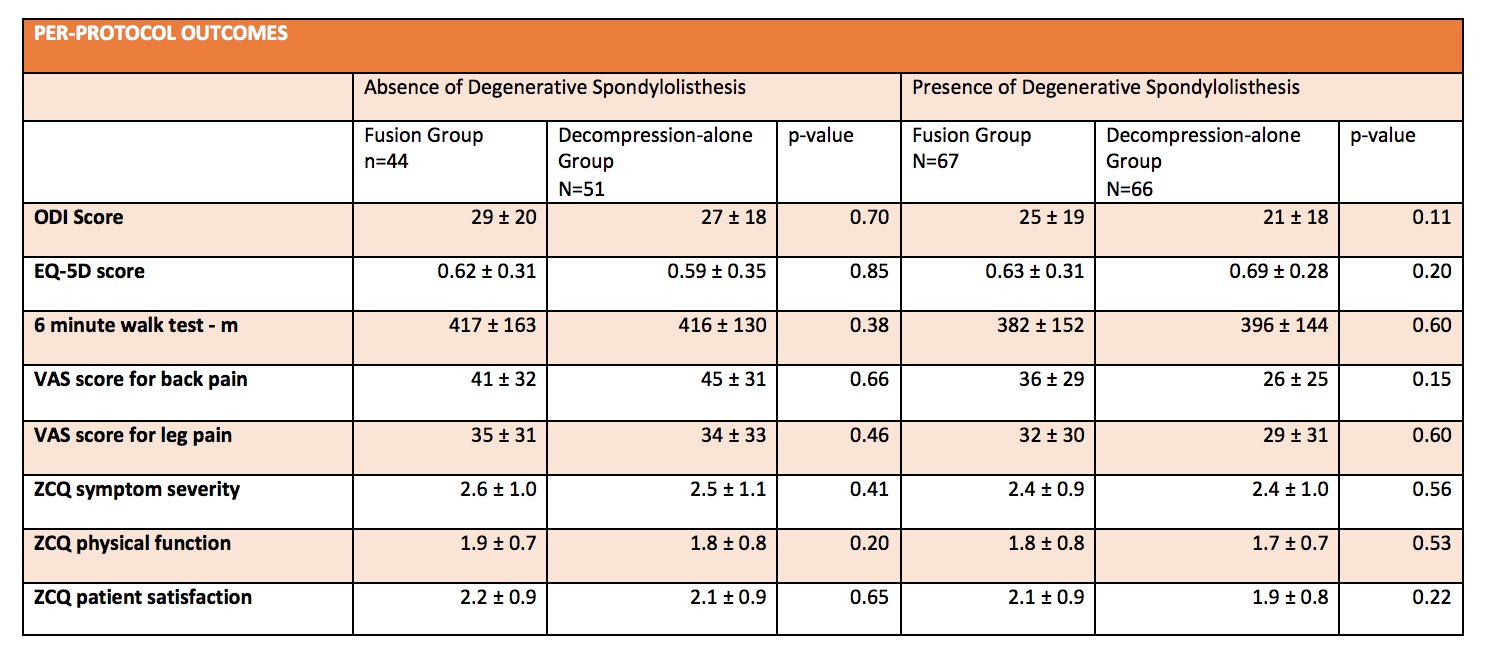
- Secondary outcomes: no statistical difference in any of the outcome measures between type of treatment and the presence or not of spondylolithesis
- European Quality of Life – 5 Dimensions; a score from 0-1 with higher scores indicating better quality of life
- Visual analogues scales for back pain and leg pain (0-100, with higher scores indicating more severe pain)
- Zurich Claudication Questionnaire (scores 1-4, with higher scores indicating more severe disability)
- Questions regarding overall satisfaction, global assessment of back and leg pain and walking ability
- 6 minute walk test (the distance in metres a person is able to walk in 6 minutes) at 2 years
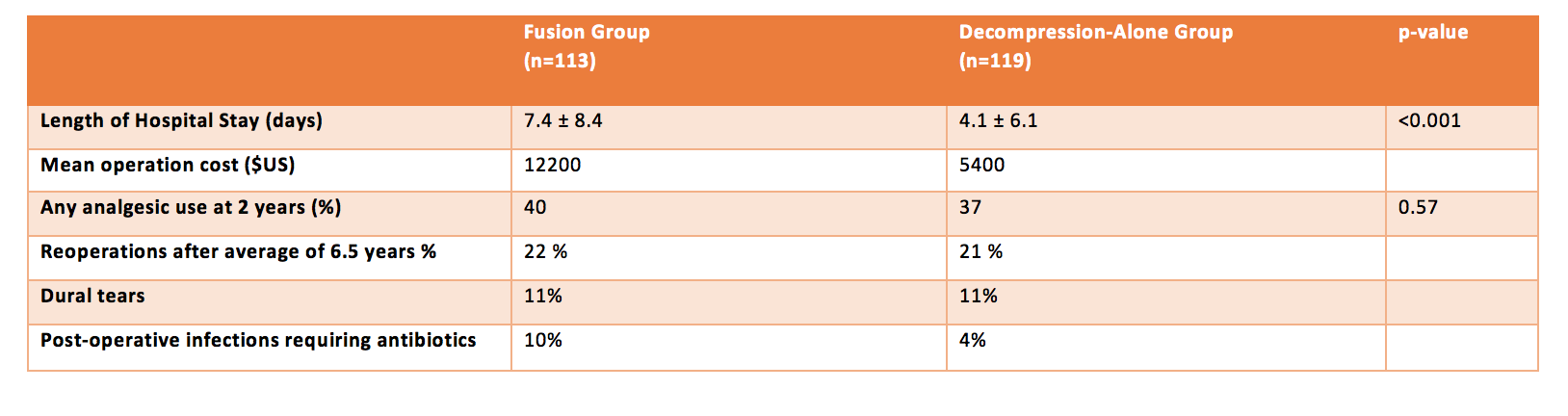
- Complications: Dural tears occurred in 11% in fusion group and 11% in decompression-alone group. Post-operative infections requiring antibiotics occurred in 10% in fusion group, 4% in decompression-alone group. AMI, CVA, thromboembolic complications were 3% in fusion group, 4% in decompression alone group
- Reoperations: 22% in fusion group, 21% in decompression-alone group
- 5 year follow up reported in a proportion of the patients: data available for 153 patients (7 had died, 1 had a stroke, 1 severe dementia, 85 within 5 years at time of publishing); 138 provided outcomes with no difference between fusion group and decompression-alone (with or without spondylolithesis) group in any of the primary or secondary outcome measures
- CT, MRI and lateral radiography at 2 years: radiology findings not reported in this paper
- Modified intention to treat analysis; 5 of the 14 patients who did not receive their assigned therapy were lost to follow-up. Of the 9 who were included in this analysis, results were similar between fusion and decompression-alone groups
- Resource use: Fusion increased hospital costs by US$6800 (from US$5400 to $12200) and length of stay from 4.1 days to 7.4 days
Authors’ Conclusions
- In patients with lumbar spinal stenosis, with or without degenerative spondylolithesis there is no difference in clinical outcome at 2 years after surgery with fusion and decompression compared with decompression alone
Strengths
- Randomised, multi-centred
- Allocation concealment
- Pragmatic design reflecting real world surgical practices
- Revision of sample size without impacting on power of study
- Blinding of the outcome assessor
- Outcomes were clinically meaningful
- Per-protocol analysis correlates well with intention to treat analysis
- Minimal loss to follow-up (93% had per-protocol analysis)
Weaknesses
- The trial was not powered to analyse differences in complication rates, however, the authors draw attention to a large analysis of registry data suggesting a doubling of severe adverse events with fusion surgery. This corresponds with a number needed to harm of 30 patients.
- Stratification by hospital and surgeon would have ensured equal allocation of subgroups to each variant
The Bottom Line
- If I were a surgeon and a patient presented to be with these inclusion criteria, I would offer decompression alone
- Unfortunately, the costs and morbidity to patients who have fusion in addition to decompression seem to be excessive AND there is no difference in clinically meaningful outcomes at 2 and 5 years and a potential to harm
External Links
- [article] A Randomized, Controlled Trial of Fusion Surgery for Lumbar Spinal Stenosis
- [further reading] Editorial
- [further reading] Quick take video summary
Metadata
Summary author: Celia Bradford
Summary date: June 28 2016
Peer-review editor: Steve Mathieu



Pingback: Global Intensive Care | The Swedish Spinal Stenosis Study (SSSS)