CATS
Norepinephrine plus dobutamine versus epinephrine alone for management of septic shock: a randomised trial
Annane et al. Lancet 2007; 676-84.
Clinical Question
- In patients with septic shock, is mortality affected by the use of adrenaline (epinephrine) alone in comparison to noradrenaline ± dobutamine?
Design
- Randomised, controlled trial
- Randomised centrally to achieve allocation concealment
- Block randomisation, stratified by centre
- Triple blinded
- Intention to treat analysis
Setting
- 19 ICUs in France
- 12.10.1999. – 31.12.2004.
Population
- Inclusion Criteria:
- evidence of infection for <7 days and 2 SIRS critieria
- at least 2 of the following: PaO2/FiO2 <280mmHg (if ventilated), urine output <0.5ml/kg for >1hr, lactate >2mmol/l, platelet <100
- and all 3 of the following for <24hrs
- systolic BP <90 or MAP <70
- administration of fluid bolus of ≥ 1000ml+ or capillary wedge pressure 12-18mmHg
- need for >15μg/kg/min dopamine or any dose or adrenaline/noradrenaline
- Major Exclusion Criteria: Pregnancy, obstructive cardiomyopathy, acute MI/PE
- 330 randomised out of 1591 who were assessed for eligibility
- The source of sepsis was lung primary in around 50% of patients (abdominal in 25%)
Intervention
- Adrenaline + placebo
Control
- Noradrenaline + dobutamine (whenever needed)
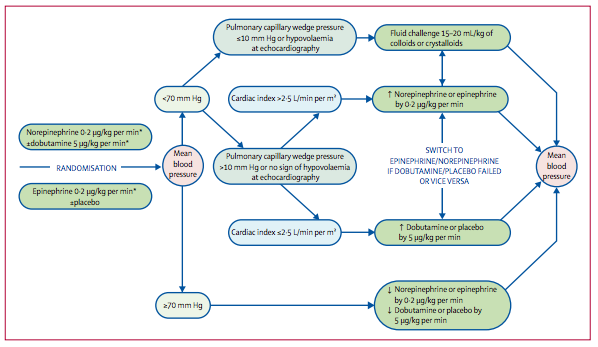
- In both intervention group and control group the use of adrenaline/noradrenaline and dobutamine/placebo was set by a pre-determined protocol shown below
- Is MAP inadequate? If yes -> are they underfilled? If yes -> give fluids
- Is MAP inadequate? If yes -> are they underfilled? If No -> check cardiac output (by whatever means) -> if ok then increase vasopressors; if not increase dobutamine (or placebo in the control group)
Outcome
- Primary outcome: All cause 28 day mortality – no significant difference
- 40% in adrenaline group vs. 34% in noradrenaline + dobutamine group, (RR 0.86, 95% C.I. 0.65-1.14, P=0.31)
- Secondary outcomes:
- No significant difference in rate of severe arrhythmias, myocardial events, length of stay and time to pressor withdrawal
- Lactate significantly increased in adrenaline group at day 1 only (P=0.003); pH significantly lower in adrenaline group from day 1-4
Authors’ Conclusions
- Physicians could use either adrenaline alone or noradrenaline ± dobutamine in patients with septic shock
Strengths
- Triple blinded
- Pre-determine protocol for use pressors/dobutamine
- Intention to treat analysis with minimal loss to follow up
- Considered specific concomitant therapy including, APC, steroids, adequacy of initial antibiotics and renal replacement therapy. These were well matched although no statistical data was conducted
- No conflict of interest declared. Supported by the French Ministry of Health
Weaknesses
- Number of patients excluded – 98 due to physician refusal and 409 due to ‘other reasons’
- Based on results found, the study had a power of 85% to detect an absolute reduction of 15% mortality, from a baseline mortality of 40%. A benefit as great as this is probably unrealistic and there could still be large differences that this trial was not powered to detect
- No mention of time to antibiotic therapy although standard treatment and adequate initial antibiotic cover similar
The Bottom Line
- There was no significant difference found between the use of adrenaline vs. noradrenaline ± dobutamine in patients with septic shock. However, the study was under-powered and with a trend towards harm in the adrenaline group, highlights the need to conduct larger studies before considering adrenaline as the first agent for the management of septic shock. I will continue to reach for noradrenaline for patients with septic shock. The study does provide some reassurance that adrenaline infusion is a reasonable alternative in the early phase of shock or in resource limited settings.
Links
Full text pdf / abstract / doi: 10.1016/S0140-6736(07)61344-0
Editorial, Commentaries or Blogs
- Catecholamine treatment for shock – equally good or bad? Lancet 2007
- Choice of vasopressor in septic shock: does it matter? Crit Care 2007
- Epinephrine: Is it really the black sheep of vasoactive agents? Crit Care 2010
Metadata
Summary author: @DavidSlessor
Summary date: 30th April 2014
Peer-review editor: @stevemathieu75