Lilja
Lilja: Cognitive Function in Survivors of Out-of-Hospital Cardiac Arrest After Target Temperature Management at 33ºC Versus 36ºC
Lilja et al. Circulation.2015, Published online February 13
Clinical Question
- In patients with out-of-hospital (OOH) cardiac arrest does a target temperature management (TTM) of 33°C vs. 36°C improve cognitive function at 6 months?
Design
- Randomised controlled trial
- Treating clinicians non-blinded
- Face-to-face follow up at ~180 days
- examiners blinded for TTM allocation but not whether or not patient was a control
- With study sample size, >80% power to detect a 10% difference between the groups based on the Rivermead Behavioural Memory Test profile score
Setting
- 5 European countries
- Out of 36 sites who participated in the TTM Trial, twenty sites completed this follow-up study
- Follow-up occurred between June 2011 – September 2013
Population
- Follow-up study of TTM Trial:
- Inclusion: adult patients who were unconscious (GCS < 8) on admission to hospital after OOH cardiac arrest of presumed cardiac cause.
- Exclusion: > 6 hours from return of spontaneous circulation to enrolment screening, unwitnessed arrest with systole, hypothermia < 30°C, suspected or known intracranial haemorrhage.
- In addition a control group was included:
- cohort of patients who had a ST elevation myocardial infarction treated with percutaneous coronary intervention
- patients matched for age, gender, country and time-point of hospitalisation
- 119 control patients
- 652 patients treated with therapeutic hypothermia included
- comparing 33°C vs. 36°C group no significant difference in co-morbidities, bystander CPR, shockable rhythm
- 342 patients treated with TTM alive at 180 days of whom 287 completed follow up
- comparing 33°C vs. 36°C vs. control group
- age: 63 vs. 60 vs. 64, p=0.04
- previous ischaemic heart disease: 28% vs. 19% vs. 13%, p=0.01
- bystander CPR: 74% vs. 84% vs. N/A, p=0.03
- 1st monitored rhythm shockable: 93% vs. 96% vs. N/A, p=.032
- comparing 33°C vs. 36°C vs. control group
Intervention
- 28 hours of temperature management with a target of
- a) 33°C
- b) 36°C
- followed by gradual warming to 37°C at 0.5°C per hour and avoidance of pyrexia for 72 hours from randomisation
Control
- Recruited from cohort of ST-elevation myocardial infarction patients treated with percutaneous coronary intervention
- matched for age, gender, country and time-point of hospitalisation
Outcome
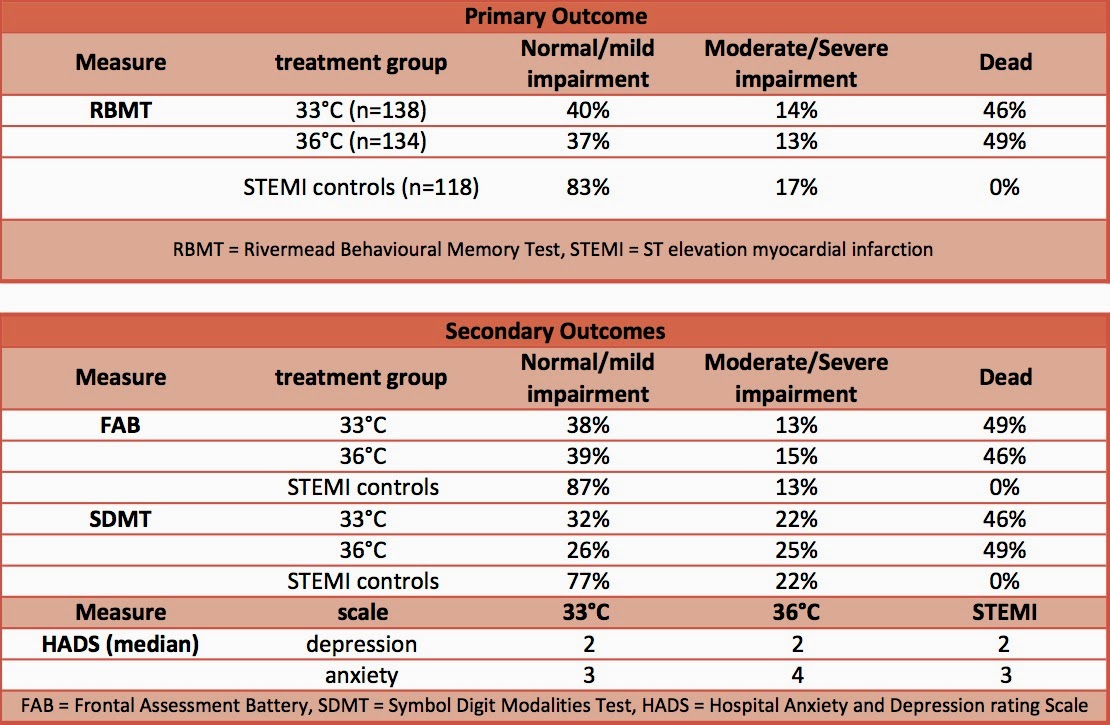
- Primary outcome: Rivermead Behavioural Memory Test (RBMT)
- no significant difference between 33°C vs. 36°C, p=0.56
- Secondary outcomes:
- Comparing 33°C vs. 36°C,
- no significant difference in
- Executive dysfunction as tested by Frontal Assessment Battery (FAB), p=0.43
- Symbol Digit Modalities Test (SDMT) assessing mental speed and agitation, p=0.31
- no significant difference in
- Including only patients who completed follow-up and the matched STEMI controls
- STEMI controls had significantly better SDMT scores than 33°C and 36°C treatment groups (unadjusted p=0.0001, covariate-adjusted p=0.002)
- No significant difference in:
- RBMT (unadjusted p=0.46, covariate-adjusted p=0.06)
- FAB, (unadjusted p=0.22, covariate-adjusted p=0.008)
- Hospital Anxiety and Depression rating Scale (HADS),
- depression, p=0.99
- anxiety, p=0.89
- Comparing 33°C vs. 36°C,
Authors’ Conclusions
- Survivors of patients with OOH cardiac arrest who were treated with targeted temperature management of 33°C vs. 36°C had no difference in cognitive outcome
Strengths
- Randomised controlled trial
- Blinding of assessor of primary outcome to TTM allocation
- Low number of patients lost to follow up
- Investigated multiple assessment measures of cognitive outcome
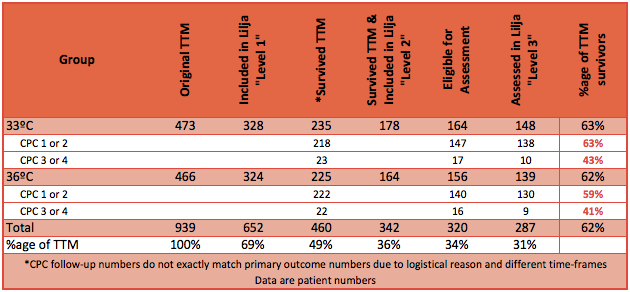
- Use of CONSORT diagram
Weaknesses
- Due to the nature of the study baseline differences in cognitive function cannot be assessed. With relatively small numbers of patients included there is a greater probability of random differences in baseline cognitive function between the treatment groups
- RBMT test may be insensitive for very mild impairment. The authors stated that the updated RBMT-3 version was not available when this study commenced
- FAB has not been validated in an OOH cardiac arrest population
- Proportionately fewer TTM patients with poor neurological recovery (cerebral performance category 3 or 4) were followed-up than those with good recovery. This will bias toward less cognitive impairment in the OHCA group compared to the STEMI-control group, but should still allow accurate comparison between 33ºC and 36ºC. It will under-estimate cognitive impairment from cardiac arrest. (see table for data)
Of note patients in the original TTM Trial had a median time of 1 minute (inter-quartile range 0-2 minutes) from cardiac arrest to initiation of basic life support. Therefore these results may not apply to patients who have a delay in initiation of basic life support.
The Bottom Line
- In patients that have basic life support quickly initiated following an OOH cardiac arrest the use of targeted temperature management of 33°C vs. 36°C does not affect cognitive function at six months
External Links
- [article abstract] Cognitive Function in Survivors of Out-of-Hospital Cardiac Arrest After Target Temperature Management at 33ºC Versus 36ºC
- [Further Reading] ESICM Summary
- [TBL Summary] TTM Trial Investigators: Targeted Temperature Management at 33°C versus 36°C after Cardiac Arrest
Metadata
Summary author: @davidslessor
Summary date: 3rd April 2015
Peer-review editor: @DuncanChambler


