Loubani
A systematic review of extravasation and local tissue injury from administration of vasopressors through peripheral intravenous catheters and central venous catheters
Loubani. Journal of Critical Care 2015; 30(3):654. doi:10.1016/j.jcrc.2015.01.014
Clinical Question
- In patients who are administered vasopressor medication intravenously, what are the published reports on local tissue injury and extravasation?
Design
- Systematic, narrative, review
- Two authors
- Initial screening of papers by one
- Full review of final papers by both with consensus resolution
- Search Strategy
- Medline, Embase and Cochrane Library
- Performed January 2014 with coverage back to 1946
- No language restriction
- Limited to human subjects
- Backward reference mapping performed
- Inclusion: case reports, case series, observational cohort studies, randomised controlled trials
- Selection: 78,671 abstracts screened, 598 full-text reviewed, 85 papers included
Population
- Inclusion: age over 18 years
- Exclusion: not cases of cardiac arrest
Intervention
- Administration of IV vasopressors via peripheral or central venous line
- dopamine
- epinephrine / adrenaline
- norepinephrine / noradrenaline
- vasopressin
- terlipressin
- phenylephrine
- ephedrine
Outcome
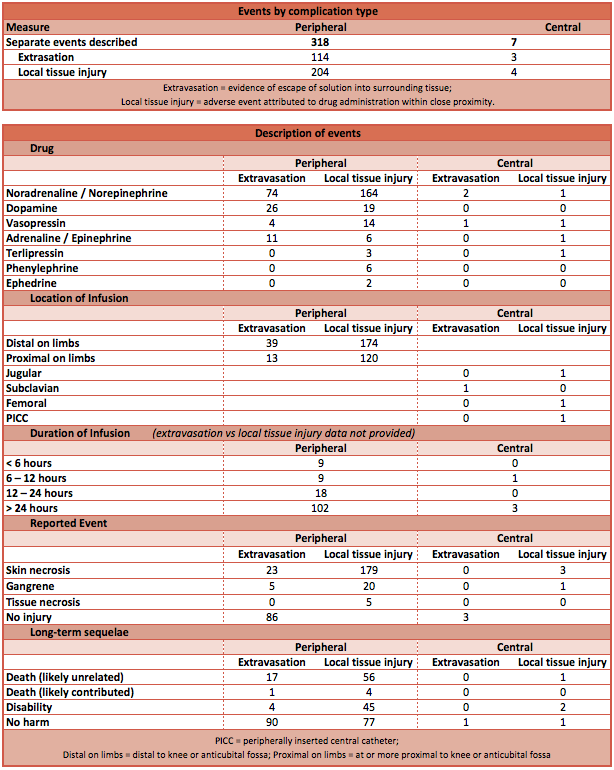
- Complications:
- Events were categorised into extravasation (evidence of escape of drug into the surrounding tissues, with or without injury) or local tissue injury (evidence of tissue injury with close association to the administration of vasopressors) – not mutually exclusive categories
- 64% of events caused local tissue injury
- 98% of these injuries were associated with peripheral venous catheters
- Tissue injuries included skin necrosis, tissue necrosis, or gangrene
- Drugs:
- Data were collected on the following drugs when provided:
- Norad / Norepi – 219 events (217 via peripheral line, 3 via central line)
- Dopamine – 36 events (all via peripheral line)
- Adren / Epineph – 18 events (17 via peripheral line, 1 via central line)
- Vasopressin – 16 events (14 via peripheral line, 2 via central line)
- Terlipressin – 4 events (3 via peripheral line, 1 via central line)
- Phenylephrine – 6 events (all via peripheral line)
- Ephedrine – 2 events (all via peripheral line)
- Data were collected on the following drugs when provided:
- Location:
- Regarding peripheral venous catheters, 62% of reported events were associated with peripherally placed catheters
- Distal to anticubital fossa (ACF) or knee – 213 events
- At ACF or more proximal – 133 events
- Regarding peripheral venous catheters, 62% of reported events were associated with peripherally placed catheters
- Duration:
- The durations of infusion prior to events were described in 80%
- The median duration was 24 hours for peripheral venous catheters and 22 hours for central venous catheters
- Most injuries occurred after 6 or more hours of infusion
- Gauge of peripheral venous catheter
- Extravasation was most commonly associated with 22-gauge lines
- The catheter gauge was rarely reported
- Long-term sequelae
- Simple extravasation was infrequently associated with harm
- Tissue injury was associated with long-term disability in 25% of described events, and death in 2%
Authors’ Conclusions
- Administration of vasopressors via peripheral IV lines for short term (<2 hours) and that are placed at, or more proximal than, the anticubital fossa (ACF) are unlikely to lead to extravasation or local tissue injury
- This should be a temporising measure during an emergency, and should be replaced by a central venous line as soon as possible
Strengths
- Well constructed literature search with clearly defined population, intervention and outcomes of interest
- Assessment of many thousands of articles for relevance
- Authors contacted for more recent articles to acquire specific patient-level data for analysis
Weaknesses
- Narrative review so exact numbers are less important
- Unable to define the denominator, so event rates or incidence of complications cannot be calculated
- Reporting bias may lead to over-estimation of risk with peripheral lines and under-estimation of risk with central lines
The Bottom Line
- This narrative review provides no firm conclusion
- From the distribution of events described, it is reasonable to conclude that the use proximal venous catheters for not more than 6 hours in emergencies, whilst a central venous catheter is inserted, is acceptable
- This work should form a base for subsequent trials if the question remains clinically relevant
External Links
- [article] A systematic review of extravasation and local tissue injury from administration of vasopressors through peripheral intravenous catheters and central venous catheters
- [further reading] Central or Peripheral Catheters for Initial Venous Access of ICU Patients: A Randomized Controlled Trial This is the only RCT identified that attempts to answer the clinical question
- [further reading] Inotropes, vasopressors and other vasoactive agents by LITFL
- [further reading] Safety of the Peripheral Administration of Vasopressor Agents
- [further reading] Risk of Major Complications After Perioperative Norepinephrine Infusion Through Peripheral Intravenous Lines in a Multicenter Study
- [further reading] Complication of vasopressor infusion through peripheral venous catheter: A systematic review and meta-analysis
Metadata
Summary author: @DuncanChambler
Summary date: 25 June 2015
Peer-review editor: @DavidSlessor


